Whenever someone in a book, movie, or show says something like, “I feel safe with you,” I cringe a little. It sounds so fake. Does that mean that person feels unsafe in most other situations? In my mind, feeling unsafe only happens when you feel that you’re in immediate danger–like narrowly avoiding a car accident or being in an abusive relationship.
However, I have recently realized I am very wrong. My own blog proves it. I have written that the world is not a safe place, and that my body is not a safe place either. We will circle back to these statements.
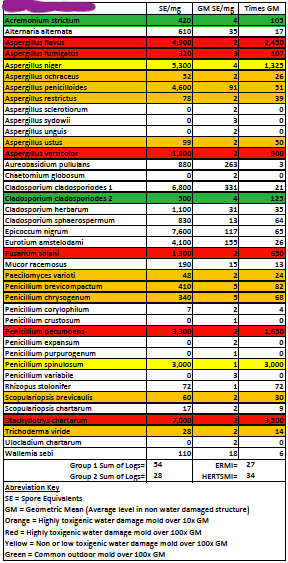
After the functional medicine doctor suspected mold was causing my symptoms, and then we confirmed that mold was present in our home, I felt relieved. There’s a reason I feel like I’m in a sharp decline and I can take steps to recover. I spent so much time in bed. I was sick, so I was allowed to rest. While part of me felt validated, another part of me doubted and questioned and researched. I don’t know if mold is indeed the original cause of my symptoms. There’s so much pseudoscience, but also new research happening.
I decided to spend two months away from my house. Luckily for me, my parents live in Oregon and have a guest room. I’m on day 57 and don’t feel any difference overall. People who’ve recovered say it can take six months or more to feel better. So, while it would have been nice to experience a dramatic improvement, I was prepared not to.
I also decided to start a brain retraining program. The first time I heard the term, I thought it sounded, well, a bit silly. I understand that neuroplasticity is real and it’s amazing, but what does “retraining” your brain have to do with recovering from mold exposure? I’m physically inhaling mold spores into my respiratory system and having reactions. Brain retraining seemed like trying to convince your brain that you don’t have a virus, or that you haven’t injured yourself. Because I was ignorant about it, it took me a long time to look into brain retraining. After I did, it took me a long time to decide to spend the money on it and commit to it. I chose The Gupta Program, which is a six-month commitment. The program is designed to address many chronic conditions that involve inflammatory responses.
With the world finally normalizing mental health, there’s lots of references around the internet to our fight/flight/freeze response and how to calm it. Typically, there’s reference to early humans running from a predator, how that served a purpose and kept those people alive. It’s the activation of our sympathetic nervous system, our stress response. We feel stressed, scared, tense. When our parasympathetic nervous system activates, our heart and breathing rates slow; we relax and recover. In the modern world, most of our threats are not physical but mental or emotional. But our bodies respond as if the threats are physical, and we have a stress response. (I am paraphrasing Session 3, Module 1 of the Gupta Program. The first three sessions are available on YouTube.)
Brain retraining can help all sorts of chronic conditions that stem from the brain creating a sympathetic response loop. In addition to genes/upbringing and stress, there’s often a physical trigger (illness, mold exposure, chemical sensitivity, injury, etc.) and the sympathetic nervous system switches on to ensure our survival. Then sometimes, it doesn’t switch off. This uses up energy and causes exhaustion. And we end up with a hypersensitive, reactive brain. The brain reacts by over triggering the nervous system and the immune system. This leads to symptoms. External stresses also feed into the immune system and nervous system responses.

So why doesn’t the brain switch off the sympathetic response after we’ve recovered or healed (or left the moldy environment)? The brain has become hypersensitive to the symptoms (the very ones triggered by overstimulation of the nervous system). The symptoms tell the brain we’re still in danger, which triggers new defensive responses. The loop, the vicious cycle, is complete. The brain has learned to overdefend. The pain signals mean there’s danger; the brain’s perception of ongoing danger leads to an inflammatory response.
The core of the brain retraining involves three things: calming the nervous system, stopping the brain from dwelling on symptoms and illness–catching yourself in the moment and redirecting–and reengaging with joy, so that you’re not “waiting until you’re better” to do things that bring you happiness.
When you realize you’re thinking about/noticing a symptom, you’re supposed to stop and tell the worried/anxious part of you, “Thank you for warning me, but you can relax and let go because….” and finish the statement for yourself. For mold it can be something like, “I may have been exposed to dangerous levels of mold in the past, but I’m safe now.” Hmmm. That sounds great if that’s true for you. If you worked in a moldy building and now you don’t work there anymore, say. But if the mold is in your house, and you still live there, then that’s trickier. I thought of “Mold is supposed to be everywhere in the environment, and it’s okay.” Or not mentioning mold at all. I know that lots of people are in my situation. The mold in their home is at “dangerous levels” for them and not for others in their household. So I’m just trying to remind my brain that I’ve lived in my house for nine years and felt fine for five of those years. Calm my brain down to the five-years-ago levels.
My job is to convince my brain that I am safe and that it’s allowed to calm down.
Part of retraining is meditating twice a day, at least. Meditation is all about letting thoughts come and go without judgment and without getting caught up in them. Being an observer of your thoughts. You are not your thoughts. They are just thoughts. Ashok Gupta, in the videos that go with the program, speaks of our dear, beloved mind. I like that idea, being so gentle and loving to our minds, rather than frustrated or anything negative.
The Gupta Program tells us to observe our thoughts with “awareness, amazement, and amusement.” Yes, it’s pretty amazing what my mind can do. In the car recently, right at the very moment I was breathing deeply and reminding myself I am safe, I imagined getting in a car accident.
My dear, beloved mind has lots of anxious thoughts. At the beginning of the program I tried out the idea that “My mind is anxious, but I am safe.” I’m okay; these anxious thoughts are just thoughts.
“But we don’t really know that we’re safe,” my brain tells me. And that’s true. That’s the problem.
Anyone who’s grown up in California knows that the threat of fire is very, very real. When I was young, my parents got each of us kids a bin and told us we could put whatever we wanted in it that we’d want to take if we needed to evacuate. Everyone in California probably knows someone who’s lost their house to “wild”fire. And it’s only going to get worse. That’s a fact. Fire “season” is most of the year, and smoke in the air is a constant summer/fall companion.
Since 9/11, I sometimes involuntarily tense or hold my breath when I hear planes. We live very near a small airport and there are single-engine planes going over our house all the time. And I know that takeoff and landing are the likely times for something to go wrong.
I could be shot in a movie theater or a grocery store or a church or a school or at a parade or anywhere anytime. This is America.
I am a woman. Since always, society has told me that it is not safe to be female. It is not safe to walk alone at night. I remember reading a list that told me I shouldn’t wear a ponytail because it’s easy to grab. That I should walk quickly and confidently to not appear vulnerable. But I can’t do that, I thought. I cannot run away or knee someone in the groin. I am vulnerable. It makes me so angry now. No one should ever be made to think their hairstyle has anything to do with someone else choosing to assault them.
Those are four examples of anxious thoughts inside my dear, beloved mind. I have never had to evacuate because of fire. I have never been near a plane crash or shot at or assaulted. But part of my brain always wants me to prepare for the possibility.
So I sit with my mind and I think, “How can I calm you in a way that you will believe?” If I can’t think “I am safe” without my brain saying, “But…” I have to find another way.
I came up with “I am safe right here, right now.” Because even if I get shot the moment after I have that thought, I didn’t know I was about to get shot. See? Totally works. It also forces me to stay in the moment rather than worrying about the past or the future.
I used that for a while, and now I am telling myself “I am safe,” hanging out in my parents’ house and there isn’t always an automatic doubt. It’s all about perception anyway. The brain’s perception of safety. Two people can be in the exact same situation and one person will perceive it as stressful or dangerous and the other won’t.
The Gupta Program isn’t helping me resolve my symptoms; it is helping me change my brain’s perception of the symptoms. I am no longer thinking things like “I am sick” or “I have mold illness.” Instead, I have but a loop in my brain. I am retraining my brain to let go of the loop. If this sounds too loopy to you, just go with neuroplasticity and calming the nervous system.
Now I’ve worked my way back around to where we began. I have written about how my world and my body are not safe. I may be able to convince my brain that I am safe in my house with the mold. But how do I handle the very real, very physical instability I live with? How do I shift my perception to one of safety when obstacles are everywhere and I keep myself from falling several times a day, every day of my life?
I don’t know the answer to this question, but I’m trying to formulate one. A big part of the Gupta Program is “acceptance and surrender” regarding your symptoms. Stop resisting them and tensing up against them. “Relax. Your symptoms are here, and it’s okay that they’re here right now.” That’s a really challenging idea when your symptoms are constant and have been for years and you just want them to go away already. I’m referring to the throat pain here, not the CP pains. Because I know the CP pains. I do feel like I’ve got a handle on acceptance and surrender to those. Most of the time. I mean, it’s an interesting place to be, trying to take care of yourself and treat what can be treated and accept what cannot, because you have to figure out which is which.
Part of the guided meditation on acceptance and surrender is, “Whatever happens, I will handle it.” On one hand, this immediately sets off the part of me that worries about the future. But on the other, I think, well, I’ve handled everything so far, so I suppose that’s true. Not that I’ve handled everything well, of course. Survived. The point is that worrying, or ruminating, doesn’t help. But knowing that usually doesn’t stop someone from worrying or ruminating. The flowchart below is beautifully simple, but it also frustrates me because reality isn’t that simple.

In my daily life, I am careful and cautious. Outside my home, I am careful and cautious and hyper aware/vigilant. Scanning for obstacles, calculating safest paths. What is it that I’m afraid of? Falling. Injury. Embarrassment. Causing a disruption. There’s lots to unpack there. But for now let’s focus on falling. I do it pretty regularly, and usually it’s not a big problem. I am to the point where if I fall outside alone, I wouldn’t be able to get up. Sure, someone would come along eventually. So that’s “handled.” (Okay, I do worry about someone holding out a hand to help me up and me pulling them down.) I worry about badly injuring my hands in a fall, especially now that I use trekking poles. That would be really rough. But it hasn’t happened yet. And if it did, somehow, we would handle it.
It is my reality that my physical instability, muscle weakness, and fatigue increase falls and risk of injury. My perception is that therefore, I am not safe. These two sentences started out as one. I had just written, essentially, that it is both my perception and my reality that I am less safe than an average able-bodied person. Then I separated the two, and I’m staring at them, wondering what to make of them. Are they true? I’m not safe from falling. Falling is scary and it is embarrassing and it does hurt–and it takes an emotional toll. But can I be someone who falls and who also feels safe?
This is the safety dance. Because if I change my perception and do feel safe, so safe and confident that I stop being cautious and careful, I will fall more. That’s not fear or worry talking; that’s reality. And though I know that if I fall, I will handle it, that doesn’t mean that I will start throwing caution to the wind and go around falling all over the place. I still want to take care of myself.
I have a disability. I am someone who falls, who holds on to things to stay upright, who needs help often. Who lives with chronic pain. I want to type “I am safe” right now, but it’s still true that I don’t feel safe a good deal of the time that I am on my feet. I don’t know how to calm my hypersensitive brain and convince it that I am safe, even with the risk of falling and injury.
There’s a lot of smiling in The Gupta Program. We breathe in and out with a smile a lot. The brain doesn’t know the difference between a real smile and a fake one, so it releases the same feel-good chemicals either way. Affirmations have been proven to help, too, and it certainly takes time to start believing them.
So I will keep going with this program, and I will smile and I will tell myself, “I am safe. Whatever happens, I will handle it.” And then I will take my poles and I will step out the door.
Right now, that’s the best I’ve got.