Last I checked in, I had gotten mycotoxin results that indicated high levels of some toxins in my body, and I had consulted an orthopedic surgeon about my right hip and labral tear.
On September 10th, someone from a certified company came to our house to do an inspection and collect dust samples to test for various molds. The dust sample is something you can do yourself and send to a lab, but I’m glad I had a professional do it and use a reputable lab. Not all labs test for the same molds, and molds can differ by region. This company uses a lab that tests for a mold common to this region that other labs skip.
Our house has no visible signs of active mold or moisture issues, but there could be mold in unseen places, like inside the walls if windows or plumbing were leaking over time. (Mold spores are microscopic enough that the width of a human hair is like a highway, so it’s easy to understand that mold spores are everywhere. Mold is only a problem when it’s the toxic kind at toxic levels.)
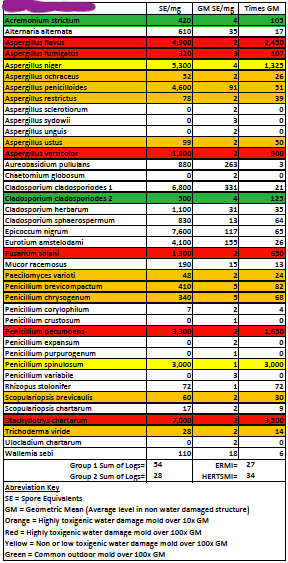
I received the ERMI (environmental relative moldiness index) results on September 21st. Here’s how the inspector explained them to me: “On the worksheet the first data column lists the mold levels in your sample, the second column is the Geometric Mean (average) for each mold as determined by the EPA, and the third column shows how many times the Geometric Mean (average) your levels are for each individual mold. The molds of concern are highlighted either red or orange. As you can see, you have many of the more toxigenic molds at elevated levels; of particular concern is the Stachybotrys [“black mold”]. It is present at the highest level and is an indication of chronic, long-term water damage. Also, you have a high level of Fusarium which produces one of the mycotoxins that you have” [based on my lab results].
These results were certainly surprising and overwhelming. Once you start reading other people’s mold stories, you learn about people who camp in tents in their backyards or leave all their worldly possessions and start over in the desert. Step one to feeling better is to remove yourself from the moldy environment. That’s simply not feasible for most people.
So. There’s toxic mold in our house and we don’t know where. The next step is to hire a certified remediation company to find and remove the mold. Remove, not kill. The EPA states, “The purpose of mold remediation is to remove the mold to prevent human exposure and damage to building materials and furnishings. It is necessary to clean up mold contamination, not just to kill the mold. Dead mold is still allergenic, and some dead molds are potentially toxic.”
On October 10th, we had a mold remediation expert come to our house. He, too, inspected inside and out and took some pictures and will send us an estimate. Searching for mold involves looking behind (removing) baseboards and other, potentially more destructive sampling. We are also waiting on results from a culture of our original dust sample to see if the mold is still active and growing.
Fortunately, the inspection company also provided us with an “effective cleaning guide” and we won’t have to move to the desert. Ninety percent of belongings are cleanable. It’s large, cushiony items like couches and mattresses that should probably be replaced. Step one was to “ban the broom,” which only spreads spores, and invest in a HEPA filter vacuum. Check.
After we figure out the source of the mold and fix it, step two is to clean. Everything. To remove the mold spores that are covering every surface in our home. I don’t want to think about that right now, so at the moment, we’re still just living in it, as we have been for who-knows-how-long.
At my August appointment with the orthopedic surgeon, he gave me the option of a steroid injection in my hip and offered to refer me to another surgeon who has experience in both arthroscopic and open techniques for labral repair and impingement repair. He told me to think about it and get back to him, but really there was nothing to think about. Yes, try the injection, and yes make the referral.
Still, I waited until a few days later to send a message through the hospital system. I didn’t hear back for a while, and what I got was another appointment with the orthopedic surgeon for the end of September. I’d hoped we’d be able to do injection locally. It seemed odd that the surgeon himself had to do it.
But drive the forty minutes we did. When we arrived, it was essentially “You haven’t had the injection yet? Why are you here?” He himself then put in the order for the injection (locally, as I thought), and the referral, as we watched. With dismay, I realized that the whole thing was a big mix up and that our appointment was over. “Unless you want me to see if I can do it with ultrasound right now?”
Yes, please. So he trundled in the ultrasound cart and someone to assist. It all seemed rushed. He must drink a lot of coffee. I did not have to get undressed from the waist down and put on a gown and climb on a table as I did for the arthrogram. Instead, I sat in the exam chair, hiked up my skirt on the right, and the field was isolated from its surroundings by draping a clean gown over the other leg. Yes, he could visualize everything he needed to without my having to go to radiology. Even I could see the head of my femur on the screen. Clean the site, spray cold numbing spray. In goes an injection of lidocaine. My whole leg (and body) tenses with the sting of the needle. It hurts inside my leg. In goes the steroid. And it’s over. (Well, there’s some grunting and grimacing and deep breaths and making sure not to look. And then it’s over.)
He asks how I feel. Um, the same except now my leg hurts because you just stuck a giant needle into it? He picks up my leg and moves it all around. Any difference now? No.
He says it’ll take up to forty-eight hours to feel the full effect, and that sometimes it can take a week. I’m flabbergasted that I’m supposed to feel immediate improvement. But that’s lidocaine’s job. It is an anesthetic. Then the steroid is supposed to reduce inflammation. So even though neither the labral tear nor the impingement change in any way with this procedure, the pain is supposed to be lessened. Instead, on the drive home I moan about how sore it is now, deep inside my leg.
I’ve started to wonder if my brain and body just don’t respond to medication in a predictable way. But then I remind myself that lidocaine has worked on other parts of my body. I had all four wisdom teeth removed at once with a local anesthetic. I had the birth control implant placed and removed from my upper arm with local anesthetic. And they really had to dig for that thing when it was time for it to come out. So. Maybe it’s just the CP parts of my brain and body that ignore lidocaine. Is that a thing? It seems like it could be a thing.
It’s been about two weeks since the injection and once the initial pain subsided, it felt like nothing at all had been done, and it still feels that way. Worth a shot, I guess. I did read a paper that reported those who responded well to an anesthetic injection also responded well to the surgery. I wonder what that means for me? I wonder if this other surgeon I’ve been referred to will have some positive stories to tell me about the dozens of labral tears and impingements he’s repaired in CP patients. I’m not holding my breath on that one.
Right now, I’m waiting. Waiting for the mold culture results and the remediation estimate. Waiting for an appointment with the new doctor. I have no idea how long all this will take. If surgery is a go, how soon will it be?
I do know that I want my home to be a safe place in which to recover. I’d love to feel like I’m recovering from the mold toxicity (CIRS) before facing surgery. I’d love for my throat not to hurt anymore and for my thumbs to work properly without pain.
If anyone wants a good laugh, watch episodes three and four of The Big Leap on FOX. There’s a dancer whose career ended because of a knee injury and a doctor comes to her office and injects something into her knee and she gets up then and there and dances without pain. Ahahahaha. In the next episode, the dancer does the injection herself. Without, you know, cleaning the area or anything. You gotta love TV. But really. It would have been nice if it had worked for me.
The first time I heard something along the lines of, “We all need to see ourselves represented,” I scoffed and thought, “No I don’t.” I was a child, and my default was to be contrary. What was the big deal about “seeing ourselves” on screen or in books? Most of the stories I read and movies I watched had nothing whatsoever to do with disabilities, and I still enjoyed them. Related to them, even. While one part of me refused to understand the significance of “representation” and what being represented meant, the other part of me pounced on anything that was remotely disability-related.
As a kid, I found Mine for Keeps, by Jean Little. Published in 1962, it was a bit dated, but it did have a protagonist with cerebral palsy. I think it was the first fictional story I read about a girl with CP.
Then there was Karen: a true story told by her mother, from 1952. I don’t remember much from this one, either, just that Karen chose clear nail polish when she was finally allowed to wear it, so that she didn’t draw more attention to her spastic hands. (Fair warning, if you do pick this one up, apparently it’s quite religious in a 1950s, Catholic sort of way.)
One book I really loved, and still love is How It Feels to Live With a Physical Disability by Jill Krementz, published in 1992, when I was eleven. Krementz interviewed a bunch of kids with a bunch of different disabilities, and in this book they tell us about their lives. Born that way or in an accident, they just tell it like it is, and I loved reading about them, studying the black and white photos over and over again. Because you can stare when it’s a photo. Scrutinize the fingers emerging from shoulders, gaze at those drooping eyes, that residual limb, marvel at the blind girl taking piano and dance lessons. So many ways of being different. A kid with CP is included, and I liked seeing my disability in there, among all the others.
Many people’s first and only cultural reference for cerebral palsy was Geri from TheFacts of Life (1979–1988). Geri Jewell appeared in the second season for twelve episodes and was the first disabled actor to have a recurring role in a TV series. (They did not renew her contract.) This was in 1980, before I was born, and I never did see the show. My first memory of someone with a disability on TV was Corky from Life Goes On (1989–1993), who had Down syndrome. At my school, “Cork” was used as an insult. I loved Life Goes On, and I remember how the show stretched my ideas about people with intellectual disabilities when Corky married his girlfriend, Amanda. Oh, how my heart ached for them as they struggled to prove they could live independently and they had a fight about undercooked pasta.
I can vividly remember from my childhood several film experiences that featured a character with a “disability.” Heidi, The Secret Garden, and Pollyanna come to mind. Both Heidi and The Secret Garden star a spunky main character with a friend who is sickly for vague reasons and who uses a wheelchair. With help from their optimistic and determined friends, these poor creatures work hard and learn to walk again. Pollyanna herself is briefly incapacitated before she, too, learns to walk again. Although these “walking again” scenes felt uncomfortable to me, I knew these movies were both historical fiction and outdated at the time that I watched them.
Then came Forrest Gump. It was 1994, and I was in the eighth grade when I went to see this film in the theater. Wow, was I surprised when Forrest screwed his eyes shut and remembered his first pair of shoes. He wore braces! Apparently, he wore them because his spine was “curved like a question mark,” which didn’t make any sense to me, but whatever. When he taught Jenny how to hang from the tree, I thought, “Now, how did he get up there and get himself in that position? And how is he going to get down?” But, whatever. Then, we all know what happened next. Forrest ran. He ran out of his braces, in a slow-motion moment. And I sat there in the dark, feeling frustrated, almost betrayed. “That’s not how wearing braces works,” I thought.
In each of these instances, disability is a plot device, a character development. Something to overcome. Triumph over. Leave behind. That’s what audiences want to see. That’s what we are conditioned to value. Imagine that’s the message you absorb about a big part of your identity, over and over again. A part of your identity that you cannot outrun.
So, what about movies about people with cerebral palsy? At least with CP, we can be sure the character will still have the disability in the end. Off the top of my head, we’ve got My Left Foot: The Story of Christy Brown (1989) and Rory O’Shea Was Here (2004).
My Left Foot is excellent, based on the book by Irish writer and painter, Christy Brown (1932–1981). I was fascinated that his CP left him with one controllable body part, his left foot, which happens to be my least controllable body part. Daniel Day-Lewis famously received an Academy Award for the role. Rory O’Shea is the story of Michael, who has CP, and Rory, who has Duchenne muscular dystrophy. They are both power chair users and live in a home for the disabled. If you know anything about Duchenne, you know this movie ends up being really sad, but before it’s sad, it’s funny. Michael succeeds at getting independent housing and a live-in (?) carer, and Rory accompanies him as his interpreter because Rory is the only one who can understand Michael’s speech. (Don’t ask me why Michael doesn’t have better assistive technology). Neither of these actors has a disability, and there was actually noise made over why actors with disabilities weren’t cast in the roles. (I wonder if anyone posed that question about Daniel Day-Lewis in 1989?)
Then there’s The Usual Suspects (1995). If you haven’t seen this movie and don’t want to be spoiled, skip this paragraph. I watched this movie as part of an American Studies class as an undergrad. I don’t know why it was in the running; I voted for an episode of The West Wing. I remember nothing about this movie except that Kevin Spacey’s character has mild CP and I was surprised and intrigued. And then in the final scene as he walks away, his arm and hand straighten and his limp disappears and he is the villain. They use my disability as a disguise. As a way for someone to commit crimes and get away with it. To make everyone think he is weak and meek and incapable because he is disabled. And he is smug and chilling and I hate this movie. This movie makes me angry. Remember how I thought that at least if there’s someone with CP in a movie, it won’t be just a plot device? At least they’ll still have CP in the end? Angry. Disgusted. Frustrated. Spacey won an Academy Award for Best Supporting Actor.
The message that movies send us over and over is that life is better if you’re not different from the norm. But difference isn’t bad. Difference is part of existence. Disabilities are part of being alive. Disabilities are normal. Let me say that again: having a disability IS NORMAL. It’s part of who we are as a species on this planet. We are born with disabilities and we can acquire disabilities at any time in our lives.
According to the CDC, the country’s largest minority group is people with disabilities, with 26% of adults having some type of disability, both visible and not. So where are we? Where are we in the stories we create and release to audiences around the world?
People who’ve always seen themselves reflected on screen have probably never thought about representation, because they’ve never had to wonder where the people like them are. (Looking at you, straight, white, able-bodied men.) If we are in any way an Other–and chances are, many of us are Othered in more than one way because most of the people on this planet are not straight, white, able-bodied men–then people will have formed ideas about our Othernesses based on representation in the media. We all form ideas, judgments, opinions based on what we consume and what we are exposed to. Books, TV, movies, music, magazines, advertisements–if you’re not represented there, how does the world know you? If you are not visible, how can you be seen?
In her 2009 talk on the danger of a single story, author Chimamanda Ngozi Adichie states, “The single story creates stereotypes. And the problem with stereotypes is not that they are untrue, but that they are incomplete.” If people with disabilities are only portrayed as the inspiring sidekick who will overcome, that leads to able-bodied people feeling surprised that people with lifelong disabilities have jobs and spouses. That limited story is why the world has people who ask utterly ridiculous questions like, “Do you sleep in your wheelchair/with your leg on?” Clearly, the general public needs to see more–more authentic and more positive–depictions of people with disabilities in all media, if only to normalize our existence.
Recently, I learned about identity-conscious casting. I watched a video essay by Khadija Mbowe who explored colorblind versus identity-conscious casting. (It is excellent and Khadija is awesome, and I really like their videos.) Much of the next several paragraphs I have borrowed from their essay.
The idea of colorblind casting, or nontraditional casting, has been around since the 1980s. Actors Equity defines nontraditional casting as “the casting of ethnic, minority and female artists in roles in which race, ethnicity or sex is not germane to character or play development.” So, if the role doesn’t require a specific race or sex, it’s open to anybody.
In 1986 (after discovering that 90% of stage productions from a four-year stretch had all-white casts) Actors Equity sponsored the first National Symposium on Non-Traditional Casting, where they focused on ethnicity (LA Times article). Nontraditional casting has been a goal since then.
In recent years, we’ve evolved to be more color-conscious rather than colorblind: “Color-blind casting (or non-traditional casting) is the practice of casting without considering the actor’s ethnicity, skin color, body shape, sex, and/or gender. Color-conscious casting, then, is the opposite of color-blind casting: taking into consideration the actor’s skin color, body shape, and other characteristics.” We as humans do see race, and “we should always acknowledge it, on or off the stage” (delshakes.org).
The second Actors Equity symposium, held in 1990, dedicated its second day to disability inclusion, as issues around casting actors with disabilities had been absent from the first symposium. While nontraditional casting had at first focused on race and gender, it began to expand, and our language has continued to evolve as well.
Now we have identity-conscious casting, which recognizes intersectionality. Not only should we always acknowledge race, but also gender identity and disability, and everything an actor brings to a role.
Victor Vazquez, founder and casting director of X Casting NYC, says, “The power of imagination is exactly what casting is. I think the American theatre struggles to understand this work: casting as imagination, casting as a culture-making machine” (howlround.com). Or as Khadija Mbowe so succinctly summarizes: “Casting is culture-making.” We create our culture through what we make, and who makes it. By the stories we tell.
When we see intersectional diversity on screen, it helps us understand what is possible, or what exists that we’ve never thought about. We don’t always know what we haven’t been seeing until we do finally see it. (For example, I had never seen a doctor wearing a hijab until Grey’s Anatomy, and it had never crossed my mind that I hadn’t.)
Let’s return to disability representation on television since the second Actors Equity Symposium in 1990. Now, I did not have cable growing up, nor was I allowed to watch much TV. Just in case I need to make a disclaimer that this is not a comprehensive discussion on disability in television, consider it made.
I remember Dr. Kerry Weaver in ER (1994–2009) and Dr. Gregory House in House (2004–2012). A forearm crutch and a cane. Just a limp they both had, just enough to make their characters more nuanced. Of course, both roles were portrayed by able-bodied actors.
Two other medical shows, one a daytime soap and one a night time soap, did hire actors who used wheelchairs in real life. Port Charles had Dr. Matt Harmon from 1997 to 2000, played by Mitch Longley. Longley became a paraplegic as a teen. I think this was the first time I’d seen a doctor in a wheelchair. He also had a romantic relationship with another doctor, a black woman. I was keenly aware that theirs was an interracial, interabled love affair, and so were the characters. (Though I’m not sure the term “interabled” existed in 1997.) Yes, they had the “Yes, I can have sex” conversation that every wheelchair user seems to be confronted with, that people seem to feel it’s okay to ask outright. Private Practice (2007–2013) included Michael Patrick Thornton as Dr. Gabriel Fife for fourteen episodes between 2009 and 2011. Thornton uses a power chair and has partial use of his hands. His character was rather arrogant and meant to be controversial. Good for them for showing that people with disabilities can be assholes, too, I guess? Interestingly, his love interest was also a black woman doctor, and they also had the “Yes, I can have sex” conversation, if I remember correctly.
Why all the medical shows with disability rep? And where are the women? And nonwhite people? That said, I was always happy to see any kind of disability representation, and watched those scenes extra closely. Grateful for every crumb. Disability representation should be so much wider than a crutch or one full-time wheelchair user as a small part of a large cast. It has always felt like tokenism.
Five years after Dr. Fife exited Private Practice, ABC brought us Speechless (2016–2019). This one is a family comedy starring Micah Fowler as JJ DiMeo. This was a big, groundbreaking deal. JJ (and Micah) has cerebral palsy and uses a wheelchair, and the premise is that JJ will have an aide, Kenneth, at school who will help him communicate. If you catch yourself thinking that someone with cerebral palsy playing someone with cerebral palsy doesn’t sound much like acting, stop and ask yourself if you’ve ever had that thought about a straight, able-bodied guy playing a straight, able-bodied guy. I was curious about the show, of course, so I gave it a try. I think I only made it through the first or second episode. I like shows that have at least a little believability at least some of the time. After Kenneth helped JJ try on clothes from the lost and found to get a new look, and they montaged through a head-to-toe cowboy outfit and several others, I just couldn’t take it. Let’s set aside that none of those brand new clothes would ever be in a lost and found. Think about helping someone with a moderate-to-profound physical disability fully undress and dress over and over again. At school. You’d both be exhausted, sweaty messes. That’s a nope for me. Even though there might have been good CP-related content in the series, the overall tone and humor were also definitely not for me.
Netflix then came out with Special (2019–2021), a show for adults written by Ryan O’Connell, who has CP, too. I heard this show was about a guy who gets hit by a car and pretends that’s why he moves differently. I really don’t like the word “special” to refer to someone with a disability, and I really don’t like the idea of lying about your disability, so I gave it a pass. Until now, for this post. I watched the pilot last night, and it was a rather awesome fourteen minutes. The show opens with Ryan face-planting on some uneven sidewalk, answering a child’s inquiries by rote (great way to get the exposition in there!), going to physical therapy, musing about his place in the disability world as an ambulatory CPer, and struggling to extricate himself from a table-and-bench situation. It was flippin’ fantastic! I have never seen those experiences (my experiences) on screen before. Wow. It turns out that seeing yourself reflected on screen is rather powerful. I hadn’t understood that as a child because I had never experienced it.
Over the last year or two, I rewatched the series Younger (2015–2021). I will not talk about the disappointing final season, but I will talk about Sutton Foster. As I watched one twenty-four-minute episode flow into another for hours, I studied Sutton Foster.
Sutton Foster is 5’9”. She is very obviously dressed to accentuate her long, slender limbs. Given that her character, Liza, is forty, trying to pass as a millennial at a publishing house in New York, her costume designer must have had lots of fun. Over Younger’s seven seasons, Liza does indeed wear some bizarre outfits. And lots and lots of short skirts and tall heels.
I often find myself watching actors do their walk-and-talks. I notice the way they enter and exit rooms, especially if they’re on their way out, and then turn and pause in the doorway. Or if they’re on their way in and they turn and close the door behind them. Then they have to turn back around and keep going. I watched Sutton Foster do all these things many times.
She is graceful, a talented singer and dancer with great comedic timing. I tried to imagine her character wearing ExoSyms or AFOs or using forearm crutches or a walker. How those elements would change her wardrobe or alter a scene. How she would look. The way she would move. A physical disability on this character would change everything, you see. The timing for everything would be different, slower. A witty line tossed over the shoulder as she leaves the room wouldn’t land the same way. Never mind sex scenes, or fancy-dress events with dancing or drink-carrying, scenes outside on grass or sand. Scenes with stairs.
Watch a show. Imagine the lead wearing braces and using crutches or a walker, so that their hands were occupied with helping them walk. How would the show be different?
In 2020, Lifetime released Christmas Ever After, starring Ali Stroker as Izzi Simmons. Ali Stroker won the 2019 Tony Award for her role as Ado Annie in Oklahoma!, becoming the first wheelchair user to win a Tony. I was excited to see her new movie because I remember Ali from her time on The Glee Project (2011), and it’s so awesome to see her in bigger roles. Is this a great movie? No, it’s a Lifetime Christmas movie, and it’s just what you’d think it is. The spectacular thing about this movie, though, is that Izzi Simmons’s disability isn’t the story. I don’t think they even mention it. There’s no tragic past accident that made her afraid to love again, blah, blah, blah. No, she is a novelist with a deadline, and that’s the story. Even though it’s probable that her wheelchair use would come up when meeting new people, I like the choice not to make it part of the story. An able-bodied actor could have been cast in the role, but wasn’t.
So how is this movie different because Ali plays the lead? There are simple, obvious adjustments, like those acting opposite her pulling up a chair or sitting on the stairs. When Izzi goes to bed, she falls asleep on top of the covers rather than taking the screen time to maneuver her legs beneath the blankets.
And yeah, just as I suspected, Izzi’s entrances and exits are a little different, a little awkward, even. But she’s startled, astonished, and acting a little odd because the man she meets looks just like the protagonist in the romance series she’s writing, so it works. She runs away unexpectedly, still talking as she goes, arms moving quickly to make a hasty exit.
This Lifetime movie got so much (positive, of course!) press for starring a disabled actor. In 2020. Thirty years after that Actors Equity Symposium focused on disability inclusion.
In September 2020, Disability Scoop summarized the findings from a report by the Annenberg Inclusion Initiative at the University of Southern California’s Annenberg School for Communication and Journalism: “Across five years of data on disability representation, the researchers said that ‘no meaningful change was observed in the percentage of speaking characters with disabilities.’ Moreover, not a single film in the 500 studied since the researchers began tracking disability inclusion featured speaking characters with disabilities in numbers comparable to their prevalence in real life.”
In episode two of ABLE, actor-comedian Maysoon Zayid is interviewed about her experiences as someone with cerebral palsy in the entertainment industry. When asked, “How do you feel about disability representation in the media? And what needs to change?” she gives a great response: “I think it’s extremely, extremely offensive when actors who are nondisabled play visibly disabled on screen. I think it’s cartoonish. I think it’s inauthentic, and I think that much like race, disability that is visible cannot be played. And the reason I use the word ‘visible,’ is that we actually have no idea how many people with invisible disabilities grace our screens. Because the stigma against stuff like, you know, mental health issues, chronic pain–it’s so strong that even stars don’t want to reveal their diagnoses. People with disabilities–we’re the largest minority in the world–we’re only two percent of the speaking images you see on TV. Of those two percent, ninety-five percent are played by nondisabled actors. That fact that. . . we are part of every single group is often ignored.” Yes, Maysoon! Nothing about us without us! Actor, advocate, and disability inclusion consultant Christine Bruno takes it one step further: “It shouldn’t be ‘nothing about us without us.’ It should be ‘nothing without us!’”
Twenty-six percent of adults live with a disability. A quarter of all characters on screen and in print should live with a disability as well. It doesn’t have to be all that they are, just as real people are complex and intersectional. It is powerful to see your own experience on screen. Especially if you don’t know anyone living with the same conditions that you do. To see a character on screen like you, showing you that you are not alone, showing all viewers that people like you exist, it normalizes our vast and varied lives.
If we saw people with congenital limb differences, for example, in our favorite TV show, we would know that limb differences aren’t so different. Perhaps then we would not have the maddeningly recent, horribly offensive utilization of the real-life condition ectrodactyly in the newest adaptation of The Witches, as an attribute to make the witches more wicked and scary. We need to normalize disabilities, not use them to promote harmful stereotypes! How did this unnecessary change to the original story go forward with no objections? Perhaps if 26% of the people involved in making this movie had had disabilities, it would not have happened.
Here’s another, very different example, just to make you think about something you may never have before. To remind us all that there are people out there, living with conditions that we may never have heard of, who deserve to have their experiences reflected back at them as valid and valuable. Approximately 1 in 500 Americans live with an ostomy, a surgically created opening in the body for the discharge of body waste. That waste is then most often collected using a pouch system. What if a character had an ostomy and a pouch that they had to monitor and change, and it occasionally came up as part of their everyday life? What if that person had a healthy sex life and participated in sports? If you or someone you love developed Crohn’s disease or ulcerative colitis and were facing an ostomy, perhaps it wouldn’t seem so foreign or scary because you had a cultural reference.
We have so far to go to achieve true inclusion in arts and entertainment. Creators of film and television have such an incredible opportunity to reach people, open minds, expand views, and increase understanding and acceptance of our amazing array of differences. It shouldn’t be revolutionary or newsworthy to hire people with disabilities and to tell our stories. We’re here. We matter. Representation matters.
Notes and References:
I know of two other movies, starringwomen with cerebral palsy, that I did not discuss: Margarita with a Straw (2014, India) and 37 Seconds (2019, Japan).
ABLE: the series Watch this series about disability inclusion in the entertainment industry for free on YT! I really enjoyed it.
Somehow, summer is almost gone. I have continued PT and some myofascial release, and I have spent lots of time resting and reading (and, let’s be honest, wasting time online). After postponing my June trip to the Hanger Clinic, I’d entertained the idea of going in August, but that’s not happening.
Week after week I went to PT without much change. But I’ve realized it’s not as bad as it was in the beginning because I can stand and chop vegetables now without needing to rest immediately. Somehow, I’ve incorporated this new pain into my life like all the others, and it’s mostly fine. Fine and simultaneously completely dysfunctional. My physical therapist encouraged me to have the arthrogram-MRI done so that I could have a consultation with an orthopedic surgeon and get their opinion regarding surgical repair. Another option is having injections into the hip for pain. That sounds awful, but better than surgery, if it’s effective, maybe…?
I was able to schedule the procedure for June 24th. I had assumed they’d be booked for weeks, but I knew it was good to get it done and move forward with treatment.
It felt weird, with my husband back in the office four days a week, to take the bus and go to the hospital alone. After my first MRI in May, I never wanted to have another, and there I was just six weeks later, doing it again.
But first, the arthrogram. I had to undress from the waist down and put on a giant gown and climb up on a table and get my feet bound together in the optimum position. It was only after my hip was bared and I was lying there pantsless that the doctor came in and explained the procedure and the risks (infection) and got my consent. Does anyone climb off the table and say no thanks, never mind, at that point?
I was very nervous, anxiety running high. When the doctor asked how I was doing, I told him, and he chuckled. They sterilized the area with cold purple stuff, put down the blue paper with a hole in it over my right hip joint. He pointed to where the injection would be and my whole right leg spasmed.
“I haven’t even done anything yet,” he said.
“I know, but–spasticity,” I answered.
The first injection was just lidocaine to numb the area. I’ll not rehash everything, but it did hurt, and I got extra lidocaine (Did you know they charge you for each dose?), and I didn’t look at the giant needle when the dye was going in. I remember, I think, that the doctor remarked about having to go around some bone. And I remember that he didn’t say anything to me before he left.
The woman assisting very nicely helped me off the table and back to the bathroom where my clothes and walking poles were. She said I could change or keep the gown on for the upcoming MRI, but that I’d be given a gown when I got there. Of course I said I’d keep the gown on, and she gave me another to cover the open back before escorting me to the MRI room. What a strange feeling, walking through the halls of a hospital in a gown, no pants, just like on TV. Stranger still to step outside, walk down a path, and enter the neighboring building.
This time, it wasn’t Jasper by himself at night in an empty hospital, but a whole different team of people who greeted me with smiles and grumbled that the previous people hadn’t already had me fill out the metal-object questionnaire. Time was of the essence with dye coursing through my hip.
I requested the headphones at the very start. I knew I would be going feet first into the tube, that the top of my head would stick out, and that I would have only one MRI instead of two back to back, this time. I knew my feet would be bound together, and I knew I’d have equipment on my legs, weighting me down. I knew I’d get through it. The tech was encouraging and kept up communication throughout the process, and I was grateful.
I counted the tiny holes in the small circle of plastic on the top of the MRI tube right above my face. I counted the nine holes over and over again in different patterns, exes and pie pieces and lines. I counted the scuff marks. I breathed and I survived.
When I was helped down off the slidy bed, I realized how sore my hip was, how I could barely walk. I got my clothes back on, my glasses and mask and sunhat and purse and poles. I slowly made my way out of the building, through parking lots, down the road, and to the bus stop. I was not prepared for the pain and stiffness and inability to move. But luckily, the bus arrived within minutes and took me almost to my front door. So grateful for that.
No one had warned me that recovery from an arthrogram could be painful. No one warned me that there would be any recovery. It turns out that having a giant needle put deep into your hip and then immediately holding as still as you can for a half hour can cause some lasting pain. It took about a week, I think, for the pain to subside to normal levels.
Results came back very quickly. I have a small anterosuperior labral tear and “mild osseous hypertrophy along the anterolateral femoral head-neck junction with decreased offset. Correlate with symptoms of femoroacetabular impingement [FAI].” Following some googling, I discovered that impingement commonly results in a labral tear. Lots of people have this condition. This condition that causes hip pain and dysfunction. Able-bodied people. It’s a little funny, right? All this time that I’ve been thinking that my right side hurts so much because of a lifetime of compensating for the left side. All this time I’ve been thinking, “Wow, I didn’t expect aging with cerebral palsy to be so far downhill so quickly.” And I have a condition that’s not even CP-related! Knowing that there’s a diagnosable, visible reason for pain is really nice, mentally.
Now, I imagine it’s possible that my CP might have contributed to the FAI in some way, which then led to the labral tear. Looking back, I think the aggressive stretching I was doing in PT might not have been a good idea, as the tear happened following that. Perhaps, I was unknowingly pushing my body too far.
But both labral tears and FAI can be surgically repaired with good results. In fact, if you fix a labral tear and don’t address the impingement, you’re likely to tear again. (I’ve read an article or two about it, so now I’m an expert.) However, there is a need for revision in a portion of the population, and revision is significantly higher for females. Hmmm. Of course, I didn’t want surgery. But surgical outcomes are better than PT alone. The prospect that, after a long recovery (and like a year or more of working up to full results), I might actually be in less pain and more functional–that my life doesn’t have to be this hard? That’s an amazing idea.
Before I jump ahead to surgery though, I need to remember that my diagnosis is a “small” tear and “mild” FAI. I imagine that diagnosis, along with my pre-existing condition would make me not a good candidate for surgery. So I have to be prepared for that. Part of me would be relieved to be told no surgery. But the other part of me really wants to know what my hip could feel like after it’s repaired.
August 18th
I’ve returned from today’s appointment with the orthopedic surgeon. The appointment was 40 minutes away, and I’m so glad my husband was able to take off work and come with me.
After we were led to our room, they came back and said I was supposed to have had x-rays, which I’d had no idea about. For a moment, I thought I was going to have to reschedule my appointment. Thankfully, imaging was on the same floor and I was able to go right in. X-rays took just a few minutes and we went back to our room that had a giant, adjustable, multi-part chair rather than a table.
The doctor pulled up the x-ray images and we could see the difference in my hip bones. My left hip is a typically shaped ball and socket. My right hip has “a very deep socket,” so that the head of the femur is hitting bone as it moves (This is the impingement, FAI). Isn’t that something? The shape of the bone itself is causing pain. Not cerebral palsy. I mean, sure, my left hip, the typical one, doesn’t always feel fabulous, but compared to the right, it’s like a 1 on the pain scale.
The impingement has been there at least since I’ve had my adult-sized body, which is just about when chronic pain and fatigue began. Common with CP, yes. I know that I’ll still have CP-related pain. But this labral tear and this FAI can be fixed. It’s a straight-forward, arthroscopic procedure. This doctor has done around six hundred, he said.
“Ever on someone with CP?” I asked.
“Nope.”
He doesn’t anticipate that there would be any problem. There is a slight chance that because of my increased tone and prior surgery in the area, he wouldn’t be able to get at what he needs to reach arthroscopically. (He might not be able to “distract” my hip.) He thinks it would be fine, as the muscle tone is coming from the brain and once I’m under anesthesia, there shouldn’t be increased tone. But there’s a small chance that he’d start the surgery and then have to stop. He could refer me to a (pediatric) orthopedic surgeon who does both the arthroscopic and open techniques, so that if arthroscopic didn’t work, he could open and do it that way. Just hearing “open,” makes my stomach sink. (More pain, longer recovery, etc.)
I think this doctor does have a good understanding of cerebral palsy. But it was still weird. You know, I start on my whole spiel, the history, the major 4-in-1 type surgery at eight, a mention of the ExoSyms, which he’s not heard of. He’s typing away. Then he comes over and moves my left leg this way and that. Moves my right leg this way and that to compare. I try to hold my leg up into his hand. That’s the whole of his physical assessment. I know he can get a lot of information out of that, and a lot out of all the images. Still, he doesn’t know me, hasn’t seen me move. He doesn’t know my abilities or capacity, what I was like two years ago compared to today. How I have literally almost no balance. And he talks about recovery time: in six weeks, I should be walking around like before. Right. Mentally, I double that, at least. He talks about being on crutches. Yeah. Mentally, I change that to wheelchair and walker. He may have noticed my eyes widen above my mask, because he did amend that perhaps my recovery may be a little different. I would have liked for him to watch my videos, pre- and during ExoSym time. I didn’t feel rushed, but I didn’t go into all that, either.
There isn’t any literature to be found on cerebral palsy and FAI. He said more than once that I was rare. But what I kept thinking is this: Cerebral palsy is a very common disability. FAI with labral tear is a very common condition as well. I’m guessing the middle of the Venn diagram is bigger than he thinks. Hip pain is such a common condition with CP, that I think many assume, as I did, that the pain must be CP related. How many of us are out there living with multiple painful conditions, when one, at least, is treatable? I know of a couple people with CP, actually, who were not candidates for surgery because of their CP. So–I was a little surprised at there only being slight hesitation on this doctor’s part. Maybe it was because my CP is mild and I seem healthy overall.
The surgeon that he could refer me to works with children with CP, so he’s more familiar with it, at least. I was pretty ready to say, “Sounds good; let’s do it.” The possibility of less pain is enough enticement to go ahead.
But I so, so dread the recovery. My only two experiences with surgery were to go in with no pain and come out with lots, and months and months of pain to follow. Logically, I know this procedure is different. I also know there will be pain and swelling, and I’m in such a bad state right now that I don’t know how I’ll be able to handle it. (I’m referring in part to the pain in my thumbs/hands/forearms, parts of my body that I’ll need to rely on in order to function.)
The other option discussed was to get injections in my hip, for pain. The procedure, he said, was similar to the arthrogram, when I had the dye injected. He said this like it was no big deal, and I let him know that it was really unpleasant, actually. I’m willing to try one, see if it helps/how long it lasts. (Could be six weeks; could be a year, apparently.) But getting injections for pain isn’t going to help the shape of my bones. Further, the older I get, the harder the recovery from surgery will be.
So. Surgery is in my future, I think. But not too soon. I’ve got to prepare, mentally and physically. Prepare my home environment. I’m already looking at toilet safety rails, shower chairs, and walkers with seats.
The doctor says in the meantime to keep up with my stretching and activity, that I won’t make the tear worse. (It seems like that’s possible, no?) Little does he know how little stretching and activity I’ve actually been doing. I like how he gave me so much credit for daily stretching. (I did not correct him.) There was a time not so long ago that I was keeping up with it.
I also need time to address the other side of my health, and I am looking into mold testing for the house and detoxing for me and trying to find reputable sources. How lovely it would be if I could feel awake again. If I could have a throat without pain again. These processes can take so much time. I feel like I need to be as strong and healthy as I can be before tackling surgery and recovery, but I also don’t want to wait months or years.
Let’s return to my adventures in functional medicine, to which I turned after years of chronic sore throat that became dramatically worse in September 2020, and ENT appointments and an upper endoscopy did not help.
First, I want to reiterate that I am frustrated by and skeptical of medicine in general for various reasons. It drives me over the edge that Western medicine takes patients in fifteen-minute increments and that nothing is done to find the cause of the illness, only to treat the symptoms. It’s just completely and utterly the wrong approach to healing someone and giving them a better quality of life.
Second, while functional medicine does try to find the root cause, those offices often don’t take insurance, making that kind of care prohibitive for most people.
Third, so much of chronic illness is unknown/disbelieved/underfunded/unresearched. It can’t be addressed in fifteen-minute increments. But just because there isn’t research to back something up, it doesn’t mean it isn’t real. It just means the research hasn’t been done.
The first time I went to a functional medicine doctor was in the summer of 2018. I was shocked by a positive result on my celiac disease blood panel. I removed gluten from my diet and looked forward to how I might feel. Many people experience a nearly miraculous improvement. Perhaps the fatigue and muscle and joint pain wasn’t all CP-related? But no, I didn’t feel any great difference. (The gastroenterologist took me more seriously in 2021 when he looked back at my original TTG Ab,IgA result of >250, the highest he had seen, he said.)
This time, with my new, local functional medicine practice, after all my intake forms and one appointment each with the nutritionist and the doctor, the doctor was pretty sure I have CIRS.
CIRS stands for Chronic Inflammatory Response Syndrome, but many doctors aren’t trained in diagnosing it (and therefore don’t think it’s a thing). CIRS is also called Mold Biotoxin Illness. Around 25% of the US population have the genes that put them at risk of developing CIRS if brought into contact with mold. From Moldy to Healthy (.com), CIRS “happens when two things occur — there is an exposure to a biotoxin, like mold, or a Lyme tick (those are the most common), or eating reef fish contaminated with Ciguatera toxin, as well as a couple more. Combined with a genetic susceptibility to being unable to clear the toxin, the body’s inflammatory response can’t shut off. This chronic inflammation impacts multiple other systems in the body, causing dysregulation everywhere.”
From National Integrated Health Associates:
“Chronic Inflammatory Response Syndrome (CIRS) is a collection of symptoms which is also sometimes referred to as Biotoxin Illness, or Mold Illness, and was initially thought to be caused by mold exposure only. However, further research indicates bacteria, fungus, and various viral infections are also implicated in the development of Chronic Inflammatory Response Syndrome.
It is quite a dilemma for both patients and physicians in dealing with such a complex illness as CIRS, which overlaps and can mimic symptoms associated with other conditions such as Lyme Disease, Ehrlichiosis and some autoimmune disorders. CIRS may often be misdiagnosed, or underdiagnosed.”
So, do I truly have tons of toxins built up in my body, causing chronic inflammation and all sorts of seemingly unrelated symptoms?
The problem is that I live in a very dry environment, where mold seems unlikely. However, mold isn’t always visible or odorous. If I’m genetically predisposed, maybe my house doesn’t have a big problem, just a big problem for me. My symptoms have gotten worse since the pandemic. Perhaps my anxiety and inability to focus and my exhaustion aren’t all because of the pandemic itself, but because I have been sheltering in my house. The pain and weakness in my fingers, hands, wrists, that I went to months of PT for–maybe it’s not from using trekking poles. It started after I began sheltering in place and wasn’t using my trekking poles at all.
Further, the mold isn’t necessarily coming from my environment. I suppose I was naive to think that food we buy in the grocery store is free of mold unless visibly moldy. It turns out that many foods, especially long-traveling foods like grains can have molds that then produce high levels of mycotoxins. See this peer-reviewed chapter, “Mycotoxins: The Hidden Danger in Foods.”
I want so much to have clear answers, to have clear next steps. I have results from a mycotoxin urine test that seem to confirm that I do indeed have high levels of toxins. Normal levels of citrinin are less than 25 (units unclear). My result was 790. Yikes, right? That certainly sounds bad.
According to the information included with my results from The Great Plains Laboratory, Inc., “Citrinin (Dihydrocitrinone DHC) is a mycotoxin that is produced by the mold genera Aspergillus, Penicillium, and Monascus. CTN exposure can lead to nephropathy, because of its ability to increase permeability of mitochondrial membranes in the kidneys. The three most common exposure routes are through ingestion, inhalation, and skin contact. CTN has been shown to be carcinogenic in rat studies. Multiple studies have linked CTN exposure to a suppression of the immune response.”
So citrinin is carcinogenic and can suppress the immune response. What else? Authors of an article in the journal Foods state, “Citrinin (CIT) deserves attention due to its known toxic effects in mammalian species and its widespread occurrence in food commodities, often along with ochratoxin A, another nephrotoxic mycotoxin. Human exposure, a key element in assessing risk related to food contaminants, depends upon mycotoxin contamination levels in food and on food consumption.”
Which foods have high levels of citrinin? According to an article from the Journal of Plant Pathology & Microbiology, “Citrinin has mainly been found in rice, wheat, flour, barley, maize, rye, oats, peanuts and fruit.” Guess what vegans eat a lot of? It doesn’t seem coincidental that three of the top foods I keep coming across in my search for citrinin information are wheat, barley, and rye. Those are also the three foods that contain gluten. Is there a connection between mycotoxins and gluten intolerance? I did find a doctor who believes so. But of course, I can find anything on the internet. Celiac disease can develop at any time in the lifespan, and although I only miss bread occasionally, it would have been really great if my celiac gene had never expressed itself. Even though I’ve adapted well to a gluten-free diet over the last three years, I eat large amounts of the other foods on the citrinin list: rice, oats, fruit. Often all of them every day!
I want to know what to do next. How to get my house (and car) tested for mold. How to get it remediated and then tested again by reputable companies. Whether or not to believe my mycotoxin test results. (In the course of doing research, I found a doctor who said not to believe urine tests.) How to change my diet if the toxic load is through ingestion. How to detox my body.
The good news is that CIRS is treatable. The bad news is that it’s not a simple process, but a potentially years-long one. I can’t find any definitive information. All that I’ve cited here is a result of my own research and not from my doctor. Most of what I’ve found is from functional/integrative medicine, and some of it is conflicting.
Again, same as with the celiac diagnosis, I feel a glimmer of hope that some of what I’m experiencing is in fact NOT related to cerebral palsy. Hope that there are steps I can take to help myself feel different, better. More energy, less pain. A slowing of this alarming decline. Is it possible?
Informal Works Cited:
Cinar, Aycan and Elif Onbaşı. 2019. “Mycotoxins: The Hidden Danger in Foods.” DOI: 10.5772/intechopen.89001
“Citrinin in Foods and Supplements: A Review of Occurrence and Analytical Methodologies.” Foods. 2021 Jan; 10(1): 14. Published online 2020 Dec 23. doi: 10.3390/foods10010014
Doughari, J. 2015. Plant Pathol Microbiol, 6:11. DOI: 10.4172/2157-7471.1000321
In my last post, I wrote about how busy April was. But I left out one of the biggest things. Last month I contacted the Hanger Clinic in Gig Harbor and asked if I could come for a couple days of additional training in June. I’ve been feeling so much stronger and have been so consistent with my practice that I feel like I can really get more out of training with an ExoSym expert now. I was excited to nail down the dates, plan an excursion to Olympic National Forest (because I hike now), and visit family in Oregon and Washington. My husband and I looked at a map and a calendar, made various reservations, and planned a two-week road trip. Yes–a trip! With travel! Outside the house! To a place where it rains!
So stoked. So excited to visit the Pacific Northwest again, and get more ExoSym training, and be in the trees, and eat food that we didn’t make. To relax and kick off the summer.
May started off well. I continued my daily stretching and strengthening and ExoSym practice. I went to a myofascial release appointment and to a physical therapy appointment. When I arrived at PT on the 5th, I heard the voice of my long-absent therapist, C, whom I hadn’t seen since November because she was recovering from surgery. This was my final appointment with my sub. He did the stretches that I can’t do alone and I showed off how much better I’ve gotten at the side leg lifts, just in the two weeks since he’d seen me last. He sent me off with excitement and encouragement, assuring me he’d talk to my original therapist–fill her in on our change in tactics and on my progress–before I transitioned back to her at my next appointment.
May 3rd. With back support.
April 19th vs May 3rd
Saturday, May 8th was a good day. We ran a couple errands and then spent the rest of the day reading on the couch. What a relief–a quiet Saturday, just as it’s supposed to be. I moved off the couch and onto the rug for a change of position. I read for 10-15 minutes with my e-reader on the floor in front of me, leaning over my folded legs, kind of like child’s pose. But I probably changed position often because I can’t last on the floor very long in any one way.
When it was time to get up, I moved from side sitting to up on all fours. POP! I felt and heard something in my right groin. And it hurt. When the pain lingered and it was difficult (more difficult than usual) to get up off the floor, I thought, oh, I actually hurt myself. It stayed the rest of that day. I used a cold pack and rested and tried not to worry.
Sunday, when I woke up and got out of bed, I immediately realized that, not only was the pain still there, it was worse. I knew that I would be breaking my ExoSym streak that day, after 52 consecutive days of practice. I knew that I would break it eventually, and that it was okay if I did, so again I rested and tried not to worry.
When Monday came with no change, I made a doctor’s appointment for 8am on Thursday, May 13th. I figured she would say, “You strained something in your groin. Heat/ice/pain meds/rest. Good luck.” But because of the upcoming road trip that we had just finalized, I needed to get it checked out. There was no way it was a good idea to use my ExoSyms in this condition. All the muscles on my right side, glutes, hamstrings, quads, the IT band, everything was gripping painfully to try to help the sharp, constant pain in my groin.
Yes, indeed, the gist of the conversation went as expected after the exam. (“Is there tenderness there?” Yes. “Here?” Yes. “Here?” Yep.) My doctor presented options and then asked what I would like to do. One option was to be sent to a specialist whose first appointment was probably months down the road. Another was to do some imaging. I picked the MRI and asked if my lumbar spine would be visible on it as well. It’s hurt 100% of the time since November and I’ve been wearing the brace every waking moment since March. It’s clearly something more than arthritis, and if there’s anything that can actually be done about it, I’d like to know.
She said, no, that she’d have to put in an order for a separate MRI for the lumbar spine, and would I like her to do that? I said yes. Then I waited all of Thursday and into Friday to hear from the MRI people.
Friday afternoon, when I got the call, she asked if I could come in that night at 7:30. “When’s your next available appointment after that?” I wondered. June 7th. The day I’m supposed to be at the Hanger Clinic. “Yes, I can make it at seven thirty.”
She then proceeded to ask me lots of questions, like if I’d ever had anything metal stuck in my eyeball. “Are you claustrophobic?” Uh…no? This is one of those questions where the answer is 100% dependent on the situation. If the space is small enough, sure, I’d panic. I hope I never discover what size that space is. She told me to remove all metal and wear clothes that are easy to take off because I will be putting on a gown. After we hung up, anxiety twisted my stomach and I watched a couple videos about what it’s like to get an MRI. If I start to feel upset, I should do square breathing and take a “wait and see approach” before pressing the panic button. Then I did a long meditation for anxiety. (I have neglected my meditation practice and it’s only occasional at the moment.)
It’s strange, but not unpleasant, to be in a nearly empty hospital. The MRI tech, Jasper, tells me that I’m dressed like I’ve done this a lot. I tell him that this is my first MRI (but I add in my head that I do understand what it means to not wear metal). It turns out that I do not have to change into a gown. While I am happy to hear that, I am very concerned that I am wearing shoes and that Jasper is not concerned about that.
He rips open a packet of foam earplugs and I stuff them into my ears. I climb onto the slidy bed and Jasper hands me “the uh-oh button,” which is actually a cord with a bulb on the end, as on a blood pressure cuff.
He says I should be as still as I can. I ask him if I’m allowed to do deep breathing wherein my belly would move up and down. He tells me to just close my eyes and breathe normally. I wonder if he’s ever felt anxious in his life.
I’m loaded headfirst into the tube. There’s a speaker near my face and Jasper asks if I can hear him. So I’ve got my uh-oh button in my hand, and I can talk to Jasper if I need to. I close my eyes and try to relax.
People with cerebral palsy often retain the startle reflex that babies come equipped with. The startle often turns into a spasm.
When the first noise comes, everything in my body clenches, and I mumble, “Holy crap. Okay.” It’s loud like a fire drill. There’s knocking and banging and beeping that constantly changes. Maybe there’s a rhythm for a while, then silence, and then more nearly unbearable cacophony.
It’s not great for my startle reflex and I really, really do not like this, but I try to breathe (not too deep) and relax. I close my eyes and attempt to focus on a song. I summon Art Garfunkel’s voice to my mind:
When you’re weary
Feelin’ small
When tears are in your eyes
I will dry them all
I’m on your side
My mind jumps ahead, garbling the lyrics.
Sail on, silver girl
Sail on by
Your time has come to shine
All your dreams are on their way
The blackness beneath my eyelids seems to be moving and I wonder if Jasper is adjusting my slidy bed. Am I moving? I can’t tell. I’m disoriented. I suddenly understand the phrase “it feels like the walls are closing in on me.” I’m really scared to open my eyes. I don’t want to know how close my face is to the plastic tube surrounding me. What if it’s too close for me to handle and I find out that this space is the space that sets off claustrophobia?
I force my eyes open. Oh, there’s more space than I remembered. It’s not so bad. I am not moving. Light is better than darkness now. Eyes open is better. Breathe.
See how they shine
Oh, if you need a friend
I’m sailing right behind
Like a bridge over troubled water
I will ease your mind
Each time the noise stops, I brace myself in the quiet for the next assault. I know it’s coming, but I don’t know when or in what manner. Each time it comes, my legs jerk. I’m trying to be still. I’m trying.
Hello darkness my old friend
I’ve come to talk with you again
Because a vision softly-ee creeping
Left its seeds while I wa-as sleeping
I grasp at any lyrics I can remember to stay focused on something.
I turn my collar to the cold and damp
When my eyes were stabbed by the flash of a neon light
I don’t know how much longer I can do this. But I cannot press the uh-oh button because that means we will stop and I will not get the images. It’s not the tube that’s the problem. It’s that I must hold still and be surrounded by all this horrible noise.
Jasper tells me we have seven minutes left. They are very long minutes. And then he says that one of the images is blurry and needs to be redone. Of course it is. How could it not be?
Finally, we are done. With the first one. Jasper sets up the slidy bed for the hip one now. He says, “Your earplugs don’t look like they are in very well. Was that really loud?”
Yes, of course it was. You told me it was going to be really loud.
He grabs a pair of headphones and puts them on over my earplugs. Well, that’s much quieter. Jasper then wraps that stretchy stuff they put on your arm after donating blood around my shoes. Yes, now my feet are bound together. Hmm. . . will this cue more panic or less? Lastly, he puts a plastic shell-type thing over my legs. More panic or less? Less. The weight is good; my body wants to relax under it rather than fight against it.
This time, I enter the giant tube feet first and stop with my head at the entrance. If I look up and back I can see a bit of the panel over the fluorescent light that is clouds and blue sky.
Here we go again. The noises are loud but not deafening now. I count the marks and scuffs I can see in the plastic. I think about all the people who have gone into this tube, scared and in pain. I think about those who squeezed the uh-oh button. I count the marks again and breathe. I am here. I am okay. I am relaxed. I am here. I am okay. I am relaxed.
My mind bounces around Beatles songs. I jump to the opening of Ragtime: “In 1902, Father built a house at the crest of Broadview Avenue hill in New Rochelle, New York. And it seemed, for some years thereafter, that all the family’s days would be warm and fair.” Now “Wheels of a Dream.” Joan Baez tries to sing “No Woman, No Cry,” to me, but I can’t focus. What if I run out of songs? You are not going to run out of songs. I can’t do this. How much longer? I am here. I am okay. I am relaxed.
I try the grounding technique of focusing on five things I can see and five things I can feel. I count the scuff marks again. I want to be done. I want to be done. I want to be done.
I do survive it and I do not press the uh-oh button. I hope that I never have to have another MRI in my life.
When I come outside to where my husband has been waiting for me, it is after 9pm. It’s just a handful of minutes later that I am safely home, in bed, where I should be on a Friday night. And it feels already like that was someone else’s life.
The results are in by Sunday, the 16th. I will be unsurprised if it says, “Everything looks good.” I will be equally unsurprised if it says, “You need a hip replacement.”
Possible anterior labral tear. Now this is ironic. I had just discovered what a labral tear is the week before. With all the chronic pain I’ve got going on with my right hip, I wouldn’t be surprised if I have that, I thought. Boom. I don’t think I’m doing “manifest your life” right. To properly diagnose the tear, I could have an arthrogram, where they inject dye into my hip and put me through the MRI again. Oh, no thank you. Let’s not if we can help it.
So PT it is, for now, with possible arthrogram and possible surgery down the line. I am sad and frustrated. I know that it’s the right call and that it’s okay to postpone the trip to the Hanger Clinic. I don’t want to go on a road trip to a forest if I can’t walk around in it.
Right now, the pain is constant, sharp. It hurts more to do any weight bearing. I need to rest after I chop vegetables. With each new pain, I think this is the one that’s too much. Too much for me to be a functional, pleasant person. That’s what I thought with my back. (Which, by the way, has some moderate degeneration. Which is a bummer but sounds about right.) This time, I think so again. This is the one that’s too much. I am tired. I would like to be put in a medically induced coma and pumped full of pain meds and sleep for a week. Then you can wake me up and we’ll reassess.
I am not in agony. I am not near an 8 or 9 or 10. Or even a 7 mostly. It’s just that it’s All. The. Time. I’ve haven’t talked about it recently, but my throat has hurt every minute of every day since September. My back every minute since November. The tightness in my neck and shoulders every minute for years. And so many other things, too. It’s exhausting.
I am not in agony. But I am also not functional. And that’s hard. I’m feeling down about it. I’m also trying to be rational and not wallow. This is where I am right now. We’ll do what we can.
Wednesday the 19th I went to PT, back with my original therapist, C. Carefully, and trying not to become overwhelmed, I related what’s happened since my last, oh-so-positive session. It didn’t seem like my two PTs had spoken about the way we’d dialed back the ExoSym practice. I hate how you have to tell everything that’s happened over months while they question you and type and you know they’re not really understanding the full picture. I told C I was getting up off the floor when my groin popped, and she mimed getting up from one bent leg and explained how that can cause hip strain. Uh, no, that’s not how I was getting up! I know it’s been six months since you’ve been here, but don’t you remember how I’ve never in my life had the ability to do that? Of course I’m not really mad at her, just sad and frustrated.
So. A labral tear does not heal on its own. Physical therapy just strengthens everything around it. I have already spent years trying to strengthen everything around it, and because I have CP, those muscles will always be weaker than an able-bodied person’s. It doesn’t look good.
I think I am at the pain management stage in my life. Give me the prescription drugs. It’s tough because pain is in your head. An amputated foot cannot hurt, for example, but phantom pain is very real and very horrible. I think my brain is doing odd things with pain signals. I don’t think my back has degenerated much more over the last six months (the condition has been there a long while), but it was only after an acute injury in November (that healed) that my brain decided to do a constant pain signal. Same thing with the throat. There is no reason we have determined that there would be chronic pain there. Hence, the desire for a coma-break. The equivalent of turning the computer off and back on again. Perhaps a chronic pain meditation retreat?
It seems like an overwhelming task to rewire the brain.
April has been so busy and so much has not yet been documented. This blog comes to you in several parts. First, let’s back up.
ExoSym Costs
My ExoSyms were paid off in February. For two Exos with two knee sections, the grand total was $21,408.00 USD. All the patient’s responsibility (no insurance), we were told. We paid half up front ($10,704). This half was for one Exo and one knee section, two separate accounts (though I didn’t realize that at the time).
At the clinic, when we handed over the first half, we (read: my dad) asked if the clinic would bill insurance for the knee sections, just to see. They did, and our insurance did cover those. So the portion of our half-up-front payment that was meant for one knee section was applied to the second Exo.
We opted for the nine-month “in-house payment plan” to pay the rest in installments. There is nothing official about the in-house payment plan, however, so I still received a general Hanger Clinic bill for the remaining amount with no mention of installments. The bill itself was very confusing to me, as it was only for the two Exos ($18,000), and stated that we’d paid $9,000, with no explanation regarding the knee sections (because of the different accounts, see?). Later, I tried to match up my insurance statement with my Hanger bill and make various seemingly random figures have meaning. The bottom line is, rather than paying another $10,704 over nine months, I paid $7,842. And by “I paid,” I mean that my parents then insisted on reimbursing me. Thank you, parents.
I am vaccinated!
As someone who works in education, I received my first dose of the COVID-19 vaccine on February 19th. My second was March 19th. I had the Moderna, and did not have any reaction other than a very sore arm. While I waited for the dreaded chills, etc. that did not come, I began to wonder whether my immune system is terrible or whether the vaccine was faulty. It turns out that a large portion of the population doesn’t have a strong reaction and everything is most likely fine.
ExoSym Practice
I have put on my Exosyms and completed a short practice session outside with back brace and poles every day since March 18th. That’s 44 consecutive days counting today. I am both proud of that and surprised by it. Some days feel good, and some days are harder. Usually, I need to recover from making it from my front door out to the sidewalk. That sounds silly, but there’s a section of incline in our path, and inclines are really hard with no ankle flexion. Some days, I can reach the sidewalk and keep walking. Do my three up-and-backs. I like to stop in between though, check my posture (using my shadow since I don’t have a mirror), do a moment of mountain pose, practice standing without weight on my poles. Some days it’s a chore, and some days it’s an exercise in curiosity. Can I feel my glutes today? Is my pelvis under me? Am I able to speed up? Reduce the strain on my forearms? Does it feel better if I try it this way or that?
April 5th
One morning my usual stretch of sidewalk was not available, so I went out to the bike path instead. In the early days, I walked this bike path toward my PT office, with the goal of eventually being able to make it all the way there and then do PT in the Exos. (Ha!) It has been many months since I’ve worn Exos on this path. The bumpy blacktop undulates up and over tree roots. Navigating such an uneven surface creates a “wobbly colt” response in me. I think it’s the lack of ankle flexion again, and the unpredictability. My body just doesn’t know what it’s doing anymore. I have been feeling so much stronger that I didn’t expect that wobbly feeling again, but there it was. It wasn’t as bad as before, but I was still a little surprised and disappointed. Not much I can do about it, though. Except keep practicing, of course.
It’s hard to tell, but the bike path on the right is a lot bumpier than the sidewalk on the left.
Back Pain
The reason I stopped wearing my Exos back in November was the back injury (from picking up something off the floor weirdly, Exos on) that turned into constant pain. An x-ray revealed mild arthritis, but that was obviously there before. I did not feel safe walking, and I knew I couldn’t add the weight and bulk of Exos to that. Bought a back support in March and have worn it almost every waking moment since. It’s great; I actually feel supported in it, and that’s a good feeling. However. When I take it off at night, I’m in more pain than I was before I started wearing it. I was afraid to put my Exos on because they would make my back hurt more. That has turned out to be true. My physical therapist figures it’s because I’m more active and suggests ice. Great. The way I roll over in bed is not helping (rolling over for this cerebral palsian is kinda twisty and archy). I tried sleeping in the brace once. It may have helped some, but I don’t like the idea of wearing it twenty-four hours a day.
I Hiked Again
On April 10th, my husband and I went to Reinhardt Redwood Regional Park in the East Bay. It was a busy spot, but a lovely day. Cool in the shade and warm in the sun. Our path was rockier than was enjoyable for good stretches of time, but mostly flat, and we did see more redwoods. I completed one mile, from our car to another lot. Then my husband went back to the car and picked me up.
Rocky, see?
April 19th
Side by side comparison
Myofascial Release Therapy
As soon as I knew the date of my second dose, I calculated the days until full efficacy and scheduled my first-ever myofascial release session for soon after. It turns out my neighbor is a physical therapist who is certified in MFR techniques, and she’s worked with many people who have cerebral palsy. I’m choosing to believe that the fact that we’ve lived next door to each other for almost eight years and I didn’t know this until I saw a flyer confirms only that I’m an introvert and not that I’m truly anti-social.
Here’s why fascia is important, courtesy of Johns Hopkins:
Fascia is a thin casing of connective tissue that surrounds and holds every organ, blood vessel, bone, nerve fiber, and muscle in place. The tissue does more than provide internal structure; fascia has nerves that make it almost as sensitive as skin. When stressed, it tightens up.
Although fascia looks like one sheet of tissue, it’s actually made up of multiple layers with liquid in between called hyaluronan. It’s designed to stretch as you move. But there are certain things that cause fascia to thicken and become sticky. When it dries up and tightens around muscles, it can limit mobility and cause painful knots to develop.
I’m pretty sure my fascia is a thickened, dried up and/or sticky, tightened mess.
I’ve had three sessions so far. My neighbor, A, doesn’t use any of those metal scraping tools that break capillaries. The release technique that she uses is gentle, skin-to-skin, sustained manual pressure. She’ll find a spot that’s tender and stay on it for five minutes or more. Five minutes. Any kind of stretching or trigger point work I’ve had so far has stayed on one place for 30, 60, or 90 seconds. She stays on a knot without forcing it, waiting to feel it release; the fascia and muscles tell her what to do and where to go next.
She’s worked on my hips, psoas, quads, and arms. Is it weird to lie in the semi-darkness while someone sits with you, hands not moving but simply firmly on a muscle for minutes and minutes? No. It’s rather nice. I am busy deep breathing, trying to relax and stay that way, and she is busy concentrating on the fascia.
The muscles of my lower body don’t want to relax. If pressure is applied, they tend to contract against that pressure in response (without my consent). During the session, sometimes I feel a muscle start to let go and then a spasm will sweep through. I hesitated to use the word spasm because I tend to think of those as painful, and this isn’t. But Merriam-Webster tells me that a spasm is “an involuntary muscular contraction,” and that is exactly what happens. The muscles do this: “Relax. Relax. Relaaax. Rela–CONTRACT!” It’s like they can’t handle it, can’t let themselves unclench. Like we have to trick them into thinking it’s safe to let go.
Sometimes I’m able to hold a contraction at bay. I can feel it wanting to take over against the gentle-firm pressure. It’s such an odd feeling. Sometimes I’ll try to stave it off, and just one leg will clench instead of both.
So my neighbor sits with me and my fascia and my contracting muscles, and she doesn’t force anything. She exists with me and my body in that time and that space and she accepts what is and coaxes small changes. And that is worth a lot.
She is also very good at trying to address my specific trouble spots. I would really like to regain my full grip strength and not have so much pain in my thumb and forearm. (I’ve been attributing this to pole use, because what else?)
Last June, I went to my first hand therapy appointment and that OT massaged the underside of my forearm and taped my thumb/wrist/forearm. I didn’t feel any different and went home without expectation of any improvement. Soon after, my neck started to tingle, and my extreme neck and shoulder tension was vastly reduced, for about a week. It felt like a near-miracle. I told A this story, and she’s worked on my forearm and taped my wrist twice, with no changes. Sigh. I think my brain must just refuse to relinquish the feedback loop: “You tricked me into relaxing once, but I know your ways now and I shall not surrender! Mwah ha ha!”
Does Anyone Know What Day It Is?
During the month of April I was busy every single weekend. Just so we’re clear, even without a pandemic, my preferred weekend activity is not having one. Along with my part-time job as a reading paraeducator, I’m also a freelance copyeditor. Sometimes, I actually get an editing job. Last summer, I became the editor for a newsletter that comes out three times a year. I’m not yet clear on its publication schedule, so when I get an email with a dozen articles attached that says, “It’s time for another issue,” I’m surprised. That happened, and then a friend of a friend contacted me to edit a dissertation, with a week turnaround time. Yikes! I said yes and then I worked before work and after work and through a weekend to finish it early and go back to the newsletter.
What’s more, my husband has recently gone back to his office two days a week instead of just on Wednesdays. So every Tuesday when he’s not at home, it feels like Wednesday. With changes at my day job, tutoring, PT, myofascial release, achieving daily ExoSym practice, TWO editing projects, AND a husband who keeps leaving the house, well, I’ve been a little out of it.
The Glute Evolution
In November 2019, I was introduced to my gluteus medius when I tried out the ExoSym test devices. In August 2020, I started to feel them really come alive. Now, I can feel my glutes working more than ever before.
My physical therapist continues to be impressed by my progress. At my last session on April 14th, he did some pretty “aggressive” stretching. When I got up from the table, I felt a bit wet-noodly. Like I really might need to sit down. That’s never happened before. But I couldn’t sit down because I needed to walk home and edit.
The combination of the stretching, the yoga, and maybe even the myofascial release already–it’s all doing something. I feel like the bit more range of motion I’ve achieved in my hips (and the added stability with the back brace) is giving me an actual stride rather than an always-bent-at-hip-and-knee clomp, clomp, clomp.
I’m using my glutes, you see. I can feel them contracting together. My backside and I have a whole new relationship. When I’m standing at the kitchen counter washing dishes, chopping vegetables, pouring something–anything that uses two hands–I am leaning my belly into the counter to hold myself up. This posture is obviously not great for several reasons. Now, I remind myself that my body can hold itself up without the counter’s assistance. I stand there and I chop up carrots and I feel my muscles holding me up. I remind myself not to cheat by resting my wrist against the counter. It takes a lot of concentration and effort to stand up tall and not cut off the tip of my finger, so it’s not an all-the-time thing yet.
But the weirdest thing is this: I didn’t realize the muscles weren’t working before. I’ve tried to articulate it previously, and I’ll do it again. My PT puts me in a modified plank and tells me to squeeze my buns together. I do, and I feel it. I’m doing the thing. But it’s like the volume was on low and I didn’t know it.
Those of you who have full use of your hands: it’s like if someone told you to lift your hands, palms down. On a continuum, A is to do it with your fingers relaxed. Z is to do it with energy through your fingers, stretched out taut. If the goal is to do Z, you do your darndest and still only make it to about G, but you think you’re at an N or an M. You have no idea what an N or M feels like, let alone Z. It’s inconceivable that Z even exists.
I know my glutes are still at the beginning of the alphabet, but it’s astonishing to discover the world of D, E, and F. I was doing yoga the other day, in my modified warrior one pose (holding on to the back of a chair). The muscles down the back of my bent leg were firing away. And I said, “Oh my god, my glutes!” so loud that my husband wondered if I was okay. Yes, just amazed.
Warrior One
The other morning I was doing my PT on the living room rug (as I have done for the last 44 days!). I was doing my side leg lifts with bent knees. These are hard. My glutes immediately start burning very strongly, and it takes a while for the burn to dissipate. In the beginning I was supposed to aim to get about a fist of space between my knees, and that was extremely challenging. It felt like an invisible thick rubber band was around my knees and I was fighting against it.
I’ve realized lately that the burn isn’t so strong, nor so immediate. And as I’ve said, my glutes are actually squeezing together. I know I’ve been getting better at these.
So I lift my leg, and it just keeps going up. I’m shocked. I stare at the space between my knees, space that I’m creating (and maintaining!) under my own power. And this is my left leg (the weaker one). I had to call my husband over to come see. My hips really are loosening up. And maybe there really is something to tight and dried up fascia limiting mobility. I was lifting my leg up higher than ever before (at least in the last two or three decades) and it felt easy enough that I didn’t realize I was doing it. Like it kept going up all by itself, without strain. Do you know how weird that feels?
My glutes are evolving, but I don’t know if my core is. All this ExoSym work is supposed to come from the glutes and the core. So far, I’m not great at coordinating all this within a step cycle, but I do try to “squish” with each step. I don’t know if my core is getting stronger but it’s just not as obvious because I’ve always had a little more control over/awareness of my core than my glutes. Or if I still have a 2019 core instead of a 2021 core.
There is still so much work to be done, so much tiredness, and a constant ebb and flow of pain from various sources. But continue to work I shall, with curiosity and gratitude.
And just so that last bit doesn’t sound too eye-rolly, know that there will be a fair bit of moaning and groaning, too.
When I arrived at my physical therapy appointment on March 31st, I had completed a short practice session with my back support and ExoSyms every day for two weeks straight. Wearing my ExoSyms for any amount of time on fourteen consecutive days was definitely a record.
When my PT called me back and I walked toward him (with back support and poles), he remarked that I was walking much straighter, my stride longer. Happy that he could see it, I explained that I could feel a difference after getting the front of the hip stretched, and that I’d been trying to maintain the looseness and incorporate the bit of longer stride into my regular gait. I also told him that I went hiking. And that I can feel my hamstrings more. One night I was sitting in bed and they were aching and seriously buzzing. Like, “Oh, hello, hamstrings. Where have you been? How nice of you to show up after forty years.”
He did the regular stretches and had me get up and walk again, with poles. “Wow,” he said. “This is a watershed moment.” Then he reassigned an exercise I’d been given and abandoned last year and enthusiastically extended my care plan until June. (It was up in March. You have to show progress or something in order to “earn” more sessions. With cerebral palsy, that is ridiculous. That’s our healthcare system for you.)
I’ve been doing my Yoga for the Rest of Us, and I think I’m actually improving. This reads as though it’s a natural outcome. I’m doing something and getting better at it. But that hasn’t felt true for me before.
I always hear how much stronger and flexible people become once they get into a yoga practice. How much better they feel. That’s the whole point, right? Those are the things that yoga is supposed to do for you. Not me. Somewhere around 2007, I remember using this DVD on a regular basis, but I never felt that the poses were becoming better, or that I was getting much of anything out of it at all. I figured that’s just par for the CP course.
But getting a good stretch at physical therapy, feeling that openness at the front of the hip, feeling that longer stride, and then doing yoga while I still feel it, it’s really helping it stay. Recently I was doing my modified sun salutations, with the seat of a chair acting as a raised floor, and I was in that lunge where you’re supposed to have your back straight and look up. Instead of, you know, being hunched over the chair trying to sorta do a lunge. And I changed one thing, I’m not even sure what, and felt this oh moment. “Oh. I think that’s what it’s supposed to feel like. I think I actually did it that time.” I DO feel stronger. My hips DO feel more flexible. The poses ARE getting better. So, when I say I’ve been doing yoga and I think I’m actually improving, it’s really more like, “I have been doing yoga and I’m actually IMPROVING!?@$#!” It’s really weird. And awesome.
When I do my PT at home, and I tighten my core (on back, knees bent), sometimes my glutes and hamstrings join in all by themselves. More on the right, but sometimes even the left side does it. It was almost startling the first time I felt it happen. Like, woah, what’s going on in there? When I’m walking with my back brace and poles, and I really succeed at engaging the core and getting my pelvis under me, I can feel my glutes and hamstrings working. I can feel my shoulders lift up and back. For a few steps at a time, it feels so different and so much better. To be both upright and moving forward at once. It’s so functional.
About fifty years ago, my parents bought land on the Oregon coast. After they had four children, they built a cabin in those Oregon woods. A true cabin, with no electricity or running water. Dad painstakingly cleared a narrow path through the woods that eventually met up with a slippery, sandy, sometimes steep trail to the beach.
We all have good memories of time together at the cabin. But there is also a consensus that “Danielle doesn’t like the cabin.” Or “Danielle doesn’t like Oregon.” For me, when I thought of Oregon/the cabin (which were the same thing in my young mind), I thought of gorse.
Gorse is a shrub with pretty yellow flowers. It’s also “an invasive species of worldwide concern” and is very familiar to me. Gorse is made of thorns. Gorse is made of thorns and tree trunks are full of sap.
My siblings might have seen adventure and opportunity. For me, the Oregon woods were an unending obstacle course. And for a kid with cerebral palsy, an obstacle course isn’t fun. The springy, uneven, unpredictable forest floor, covered in twigs and branches and vines and rotting stumps and ferns and gorse. And what is there for me to steady myself with? Trees covered in sap.
I did not explore with joyful abandon. Climb from stump to stump to stand tall atop the biggest one. Build forts. Leap across streams. The forest wasn’t accessible to me. It was an environment that was difficult to participate in, to be a part of.
I’m not exaggerating when I say that my most vivid memory of being in the woods around the cabin is of falling, and lifting my hand to pluck the gorse thorns from my sticky, sap-covered palm. I do have many good memories, too, but the strongest one is landing with a sudden rustle-thud that only that forest floor can produce, and assessing the damage.
Even the ocean, when we finally made it down to the beach, wasn’t something I loved. Navigating sand is nightmarish, and the water was cold. Then I had to climb back up the steep, slidy trail. With wet sand in my shoes, chafing my toes.
It might only be because this picture exists, but I swear I remember looking over the edge of the red, flowered rim of that backpack as my dad slid, unintentionally, on his bottom down a section of trail. 1983.
But, look! I used a shovel. Notice how hard I’m holding on to it. 1983.
Apparently when I was ten, I could kind of do that one knee up, one down pose and not tip over. My toes dug into the sand, even when it was hard packed. That outfit, though. Rest assured that my socks matched my scrunchie. 1991.
I think the last time I slept at the cabin, I was in my early teens. When my sister got married there in 2009, and many of the guests went down to the beach, I did not even attempt to go. When I brought my own husband to see the cabin years later, he too, went down to the beach while I waited, safely seated, and imagined his trek through the trees.
When given the option to be outside or inside, I’ve mostly chosen inside. Inside is safer. Inside is easier. (Okay, both times I’ve needed stitches were inside incidents. Nowhere is safe. Just safer.)
But I also LOVE the forest. The roaring quiet. The dim coolness. The alive stillness. Trees feed the soul. You are compelled to breathe deep of the oxygen. Compelled to speak softly inside the majesty.
I don’t remember my first accessible hike. Not that there have been so many of them. Palisade Falls near Bozeman, Montana, in 2004, maybe. Then Glacier National Park, on a raised wooden walkway. Being able to walk beneath and among the trees without expending all my energy and concentration on staying upright is spectacular.
Sometimes I feel like I need to just be with the trees.
Glacier National Park, 2013
Prairie Creek Redwoods State Park, 2020.
No tree is too big for a hug.
My husband, he takes me to the trees.
Wanting to take me to the trees again, my husband found Roy’s Redwoods Preserve in Marin County. It was my second spring break of the pandemic, the second year we did not go on a weeklong trip, so a day trip we took. Now, it turns out that the name is a bit of a misnomer. While there are some redwoods in this preserve, we did not reach a place on the trails where I was truly surrounded and sheltered by them. No alive stillness for me that day. Instead, I experienced a different kind of aliveness altogether.
Friday, March 26, was my first real outing with both my back support and my trekking poles. I also wore really supportive shoes with a stiff sole. This was my first trail that was not officially deemed “accessible.” We chose Roy’s Redwoods Loop Trail over the Meadow Trail, because I wanted redwoods, not meadow. The trail started off fine, narrow, but flat. Soon, though, I encountered rocks jutting out of the packed dirt, and inclines. And inclines with rocks. I surprised myself by navigating up those uneven inclines and over those jutting rocks. “I did it!” I said, like a toddler learning a new skill. My husband stood near when I hesitated, ready to assist while I attempted different footings and pole placements, but, I did it all by myself.
I wondered how much harder it would get, and how much more I could actually do. And how I was going to get back down. This loop was not small and we were not planning to do the whole thing; was it already time to abort mission? But I wanted to see if I could get to the redwoods that were supposed to be on this trail, so we kept going. For the record, here’s its official description: “For a peaceful getaway, meander down Roy’s Redwoods Loop Trail.” My husband meandered peacefully, while I worked through the most challenging terrain of my adult life. The pictures don’t do it justice. I didn’t think to pause for photos on the hard bits because I was a little too busy not falling.
This is narrow. And not flat. And do you see that root?
Eventually, we emerged from the trees and found ourselves on the side of a hill. I looked down to my right and up to my left and realized I had hiked up a hill. We kept going for a while longer. We did not reach the redwoods, but we did end up meeting the Meadow Trail, so we did not have to retrace all our steps (some of which I’m pretty sure I couldn’t have handled going down).
Do you see how I’m in the middle of a HILL?
The Meadow Trail was easier, but we still had to hike in a downwardly direction. Down is much more difficult. Instead of leaning up into my poles and heaving all my weight onto them as I step, I had to place them down in front of me without falling forward with them. There were a couple of legitimately scary moments for me, but I made it down all by myself. I hiked. I’m a hiker.
We made it back down the hill. I am standing up tall in a circle of redwoods, with no weight on my poles.
I would not have been successful if we had tried to hike with me just holding my husband’s hand. I would have pulled his arm, hard, the whole time, and still not have been able to do it. Without the poles and the back brace, it would have been truly impossible. I would not have even attempted to climb over/around that first jutting rock, because I would not have been able to stay upright. Good poles, good brace, good shoes. I have found a combination of tools that give me what I need to be able to do what I cannot do alone. To my knowledge, no doctor has ever suggested back support for me. I have been given exercises to strengthen my outer hips, to combat my side-to-side shift, since toddlerhood. My entire life–Strengthen those hips! Don’t let that hip drop! It turns out that stabilizing my trunk helps so much, enabling me to focus on the glutes. Yes, I’ve been doing my glute exercises consistently for months as well, but I can’t help but wonder if we’ve been going about this whole thing backwards. Strengthen hips=stable core? Or stabilized core=ability to engage other muscles.
If you have cerebral palsy similar to spastic diplegia with hip drop, I say try some back support and see what it feels like.
I have accomplished many things I’m proud of. Not many of those are physical achievements. Physical success is not something I often experience. As I continued to navigate obstacle after obstacle on that trail, under my own power, I suddenly understood how doing physical things that are hard can be almost…fun. Meeting a challenge. Here is a time when the term “physically challenged” is appropriate. I was physically challenged by that hike, and I succeeded. And I liked it. I want to hike again. With more redwoods next time.
I’ve mentally composed bits and pieces of a blog entry so many times that it seems as though I must have already written it. But I haven’t, so here we are, as I finally buckle down to write during my second spring break of the pandemic.
When I first got my ExoSyms, I was told it would take one to two years before I was using them to their full potential. I liked the idea of marking time, tracking that progression, until I could say, “It’s been two years and look at me now!” But I’m nine months in, and I don’t feel like marking time anymore. I’m no longer going to put the number of days in the titles of my posts. Progress is not linear, and there’s no endpoint. I keep thinking, What if they’re not for me? What if I just don’t progress beyond walking on a flat surface with poles? Maybe my body truly cannot use them to their full potential and it’s a case of too much, too late.
I’m part of a Facebook group for women with cerebral palsy. Recently, someone wrote about how she used to walk independently and now she needs a walker. She fights the feeling that she just needs to “try harder,” that she shouldn’t take twice as long to clean the house and use twice as much energy doing it as she used to. Others chimed in, feeling the same. The decline is real. And it’s making itself known to me in very real ways. If ExoSyms had been available to me when I was twenty or twenty-five, before all the chronic pain and decline really took hold, maybe I could have really used them then, and extended my peak quality of life. But now? I just don’t know if I can do it.
The pandemic certainly hasn’t helped. It’s had a physical and mental effect on all of us. Maybe there’s a small group who were really able to use the time at home to cook well and do yoga and take up running. For the majority of us, our physical activity has plummeted and our time in front of screens has skyrocketed. Of course it’s not good. I’m not sure that I can ever achieve my pre-pandemic level of activity again. In 2019, when I first started using trekking poles, I was delighted with how they helped me, what a great option they were for longer distances. Now? Now I need them. I have gone from walking independently to using a mobility aid, just like so many others with cerebral palsy.
With PT, I had left off with my therapist at a loss and ready to let me go for six months. Instead, I decided to keep going. When I returned mid-February after a month away, not having pursued more x-rays or the facet block shot as he suggested, I said that I think consistent therapy is a worthwhile thing. My cerebral palsy is not going anywhere, and I can get stretched with a therapist in a way that I simply cannot replicate at home. That session was the first time this therapist had ever really explored my increased tone and decreased range of motion, I think. (He has taken over from C, who is recovering from surgery, and we had been focusing on core and glute strength and lumbar issues.) So this was for him an introduction to how my body works. He realized that, yes, actually, I can benefit from passive stretching. There was a “wow” moment, as in “whoooa, that’s tight.” Yes, I thought, now you understand.
He did stretches that I can’t do alone and encouraged me to try them with assistance from my husband. So, I’m back to going every two weeks. We’ve even done a couple ultrasound sessions on my right piriformis, which is more often painful than not.
Also in February, I finally made myself get in touch with Ryan at the Hanger Clinic and let him know what’s been going on with my back, and that I hadn’t walked in my ExoSyms for more than three months.
“So you’re really starting over then. That’s okay,” he said. It’s not entirely true, as I’ve tried hard to keep up with strengthening my glutes and core, and I hope I’ll have at least maintained what strength I had in the fall. Ryan suggested some back support and told me to practice walking fifty feet five times at a stretch and then take the Exos off. (Rather than trying to wear them for hours at a time, navigating around furniture, etc.) He sent me four brace options. I sent those on to my physical therapist, and ordered the winner.
My new brace arrived on March 8th. This is the second time that I’ve made an assumption about physical aids and been proven wrong. The first was about the poles, and how I thought they wouldn’t help and just be a tripping hazard. With this brace, I had wondered before if back support would help, so I was open to trying it right away. I still figured it was likely that it would just be uncomfortable and not do much.
I have to lie on the floor, bend my knees, and make sure my back is flat before I strap myself into it. The first time I did it, and got myself back to a standing position, I said, “Whoa.”
This thing holds me up. It holds me in. It’s there, supporting me. Hugging me so firmly. It doesn’t let me take steps the way I usually do. It’s amazing to realize how much my lack of trunk control must be affecting my gait, my alignment, my whole body. Because I don’t really feel like I do lack core stability. It’s another “Oh” moment. How can I know what stability feels like if I’ve never felt it? This little bit of stability afforded to me is like a glimpse into another world.
The worry, of course, is that my core will become weaker as I rely on the brace. I don’t think this will happen. It’s more like it’s giving me a continuous awareness of my core. Like when a therapist or instructor touches your abdomen and says, “Tighten here.” It’s easier to do it when you know where to focus, or when you have something to tighten against. The brace feels similar to the super-tight belt and pole combination, used during Hanger training week to teach me how to “squish” with each step. I think for me the belt did more than the pole. As soon as Jared took it off, I didn’t feel my core as well, couldn’t tell whether I was really squishing.
I may be feeling a further benefit as well. It’s a little like having my own personal weighted blanket on me at all times. I’ve never tried a weighted vest, used with kids on the autism spectrum, but I’m guessing this is similar. It’s the firm hug that calms the nervous system. It’s Temple Grandin’s squeeze machine. I’m not saying I’m completely calm now, but I can say that I like wearing this. If you have anxiety, it’s an inexpensive option to experiment with. Yes, it can be uncomfortable. Yes, it tends to ride up and need readjusting throughout the day. Yes, it makes wearing clothes interesting. And yes, it’s going to be way too hot in another week or two. But–I like it.
I’m tired of letting the pandemic get the best of me, and with the stability for my back that I needed, I’m trying, once again, to increase my physical activity. I returned to three seated workouts I like on YouTube. I find these extremely challenging once they get going, and have started again with only fifteen minutes. The only time I’ve made it through an entire workout (several years ago), it took me and my husband months to work up to it! All three of these workouts are truly gems. Along with some schnazzy workout gear, they all feature people of different sizes and races and abilities. Two of the workouts have real, live people with cerebral palsy. It’s truly an awesome sight to behold. As I feared, however, these arm workouts are really, really hard on my tight neck and shoulders, so they are not for every day.
As such, I’ve also returned to my trusty Yoga for the Rest of Us DVD that I’ve used intermittently since 2006ish. I’ve been doing it before work. This is not as impressive as it sounds, since I no longer have to be out the door at 7:30 am, but still.
I’ve also been taking more walks in my brace and with my poles. Instead of twenty slow, careful, cautious minutes worrying about my back and trying to engage my core, I can now do 60+ slow, careful minutes engaging my core.
A week after getting my brace, Monday, March 15, I put on my ExoSyms to try my first true practice session since November 1st. I no longer walk across the house without poles, instead making sure my poles are right there when I need to walk to the front door. Day 1 was hard. My right hip was so sore and tired. The “Is progress even possible?” thoughts resumed. I did my three up-and-backs along the sidewalk and made my way back to my front door, ready to take them off. The next day, I did it again. The third day, I reported back to my physical therapist and got stretched. Thursday and Friday, I put them on again. It felt like a good week. At least I was doing something with them on. I had this realization: I need to practice on Saturday too. No more giving myself the “day off.” I don’t need a whole “rest day” after only ten minutes of dedicated practice. After all, I’m not pushing myself or taking risks or hurting my back now; I’m slowly building endurance. This is something that needs to happen every day. That’s all there is to it.
Saturday morning came, and I fully and absolutely did not want to strap myself into my four pieces of heavy carbon fiber and take myself outside. Not for the first time, some of the most relatable lines from Leonard Bernstein’s MASS came to mind, from “I Don’t Know”:
Why I drift off to sleep
With pledges of deep resolve again,
Then along comes the day
And suddenly they dissolve again.
I don’t know…
So many pledges of deep resolve we make, only to let them go when we simply would rather not do the thing. My husband said, “You just have to do it anyway. Even as you’re telling yourself you don’t want to, put them on.” He was right, of course. So I put them on anyway on Saturday. And on Sunday. And on Monday, the 22nd, something happened. It’s always hard to know if I’m using my core and squeezing my glutes and “loading the devices” all correctly, all with the right timing for each step cycle. I try it different ways, not knowing which way is right. I remember Jared telling me to kind of lead with my pelvis, but how do I do that and lean into the knee cuffs properly (load the device)? Also, when I’m stretched well in PT, I can actually feel a little looser at the front of my hip for a while. Which means that I have more range of motion in my step. I can actually straighten the knee before the foot comes off the ground to swing through, rather than keeping my knee slightly bent throughout. At least, that’s what it feels like. I don’t know if that’s what’s actually happening.
So, right now I have a smidge longer stride that I have to figure out how to coordinate with the Exos. Do you know how weird it is to suddenly have a longer stride? It throws everything off if you actually try to use it. But looser hips and a longer stride are very good things, so now I’m trying to see if I can keep it going until my next professional stretching session on the 31st. I’m out there in my back support and my Exos, practicing, trying to incorporate this new stride and coordinate everything. And suddenly I’m walking faster. It’s a week after I’ve started walking in them again, and I’m startled to realize I seem to already be going the same speed I’d built up to last fall. Maybe even faster?
It felt like I was just walking. It felt really good. There’s no way I can know where I’ll go from here. If or when I’ll progress beyond using poles on a flat ground. All I can do is keep practicing.
Here’s video from March 23rd, and a side-by-side with the last video we took before the back injury last fall. Any difference? Hard to tell.
On my fourteenth birthday, my mother asked if I felt like I was fourteen. “I feel like I’m forty,” I intoned. Teenangerhood is such a joyous time.
1995. Note the plastic spider on the corner of the cake. Yes, I did crop my brothers out of this photo.
Now that I am forty, I can say, like everyone else who’s made it this far, that it doesn’t feel as old as you imagine it will as a kid. Sort of. It’s that whole “the days are long, but the years are short” thing.
I remember having energy once. It was a Wednesday. It must have been over a year ago because I was working outside of my house. I felt so different from my usual self. More awake. More alive. I was functioning on another level of existence. I was more patient with my students. And it felt easy to be patient, not like I had to stop and reword my response into something that didn’t sound short or exasperated. I enjoyed my students more. I smiled more because I felt happy. Wow, I thought, some people feel like this most days. The ones who are excited to wake up and go to work in the morning. Who seem so genuinely happy. I don’t dislike my job. It’s a good fit for me, and there are moments I truly enjoy. But no one would ever say that I am energetic or enthusiastic. I make it through my day.
But that one day. That day I got a tiny glimpse into what life could be like. People who have drive must feel like that. People who work so much and sleep so little. People who ACCOMPLISH THINGS, who dedicate their lives to their calling. Booker T. Washington. Ruth Bader Ginsburg. So many people. They must be people who have energy. They operate on another level.
I don’t know what was different about that day. Did I just get really good sleep? Have some kind of spike in the good hormones? Whatever it was, it was an amazing experience.
Now it’s over a year later, and I’ve become one of those patients. One of those patients who says it hurts, but no one can find anything wrong, so they send me back where I came from. On my video call with the GI doctor, he wanted me to tell him an exact number of times I’d had heartburn over two weeks. I didn’t have that number, but it wasn’t my main issue. I told him it’s improved with diet changes. He says my endoscopy results from October look normal. (Even though it says reactive gastropathy with mild chronic stomach inflammation right in my records. I guess mild inflammation is just fine.) He says it doesn’t sound like reflux. I started tracking my food and my symptoms so I can give the next doctor a flippin number. I’ve eaten chocolate and other acidic foods and had heartburn about half the time, so I stopped again. My eyes are glazing over even as I type this. The point is, he sent me back to ENT, a different one this time, because I don’t have any symptoms of a GI issue that would cause throat pain, so maybe it’s a sinus issue. She prescribed a bunch of antihistamine type stuff to try even though she couldn’t find much of a problem.
On the cerebral palsy front, my physical therapist doesn’t know what to do with me either. In January, I brought in my TENS unit so he could show me how to use it on my back. I’ve had it for a long time, but I don’t like the feeling of the sticky pads and it seemed like a lot of hassle for not much. Plus electricity scares me. After trying it out and reporting back (it maybe kind of worked if I meditated and used the heat pack all at the same time), he suggested I look into the facet block shot in the spine that my GP mentioned. Then he said I could take a break from appointments and get a new referral in six months, or see him in another month if I wanted to keep it going. Basically, “I don’t know what to do to help you. Your call.” I made an appointment for a month later.
For the last three months, I’ve stayed out of my ExoSyms and tried to give my back “a chance to heal.” After the initial injury improved a little, my back has stayed the same. As I’ve said before, the pain isn’t bad, but whatever is going on is decreasing my function quite a bit, so it doesn’t feel safe for me to use my ExoSyms. But it’s been so long, this might be my new normal. I’ve got to just work with where I am right now.
So I put them on and I stood in a doorway for ten minutes. The next day, I did it again. Stood there. For ten minutes. I am taking short walks outside without Exos, slowly and carefully with my poles. Trying to engage the core. Feeling so far from what I did before the pandemic. Still a little bewildered with where I find myself.
I’m ready to go back to a functional medicine approach. Silly me to think that some antibiotics for strep in 2019 or some reflux meds in 2020 would help me feel better. I’m ready to look at other modalities for CP as well. Chiropractic work scares me. Maybe some myofascial release? I’d really like to have the vaccine before I commit to one-on-one bodywork though. So who knows when that will be.
Here’s what my birthday looks like this year. I’m also getting some super nice socks, but I’m waiting until the actual day on Tuesday to open those.